Hit the Box! Educational Resources for When Boarding Gets the Best of You

Below you will find a weekly series of educational resources and a case bank that can be used on shift during times of boarding.

Week 15: Hemostasis Sutures


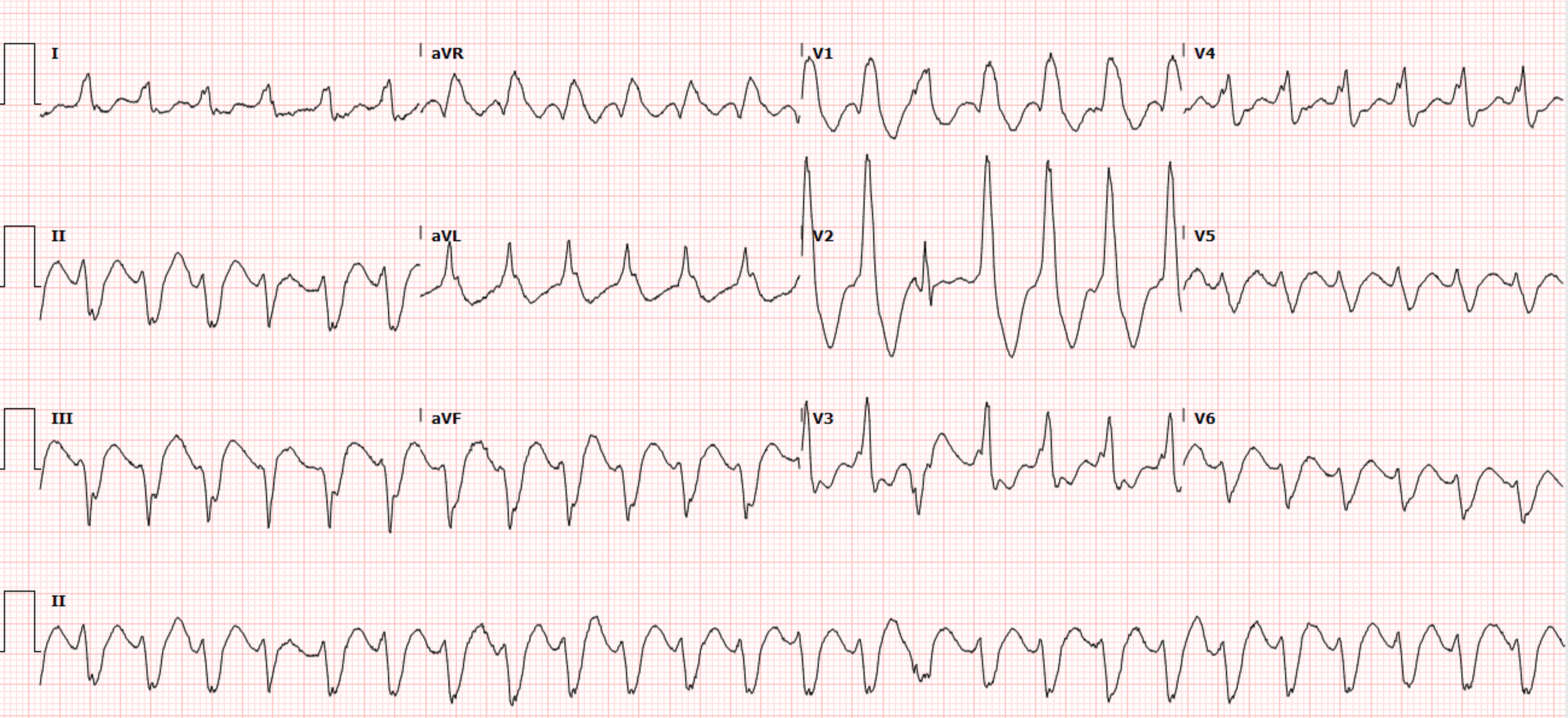
Week 15: 26 y/o M without significant medical history who presents for sudden onset palpitations and shortness of breath.

In the times of paper charting, new patients would show up in a file box in A/B/C pod - “Hitting the Box” is our colloquial saying for picking up new patients.
Click here for Link to Case Files
Instructions - These cases are meant to be presented to the learner over a longer period of time. The objective of the case administration is to force the learner to task switch and to essentially add an extra virtual patient to their list of active patients.
Start by allowing the resident to collect a history and physical and order some labs. Allow some time to pass and then provide them with the lab results (can time this such that it forces them to task switch). Discuss additional diagnostics and therapeutics and then allow the case to unfold until they ultimately disposition the patient. You can debrief on the content at an opportune time when the resident has time to digest the learning points.

The Archives - Previous weeks resources
Link to One Drive - Boarding Educational Resources
Procedures
Week 1: EJ Placement
Week 2: Peripheral IJ
Week 3: Subclavian Line
Week 4: Supraclavicular Line
Week 5: Femoral Line
Week 6: IJ Central Line
Week 7: Hemodialysis Catheter placement
Week 8: Abscess I&D Loop Drainage
Week 9: NailBed Laceration Repair
Week 10: Bartholin Gland Abscess Drainage
Week 11: Lateral Canthotomy
Week 12: PTA Drainage
Week 13: Tube Thoracostomy
Week 14: Pigtail Tube Thoracostomy/Pneumocath Placement
Week 15: Hemostasis Sutures
Week 16: Sutures for Friable Skin
Week 17: Lumbar Puncture
Week 18: Nerve Blocks - Radial, Median, Ulnar
Week 19: Nerve Blocks - Foot and Ankle
Week 20: Nerve Blocks - Face
Literature
EKGs
Week 1 - Clinical Setting: 78 y F with history of a-fib, CHF, CAD presenting with sudden onset of generalized weakness and dyspnea. HR - 180, BP - 90/53, RR - 16, SpO2 - 94%, Temp - 99 F
Week 2: Clinical Setting: 48 y M with schizophrenia found collapsed in stairwell of hospital garage, now complaining of “can’t breathe.” HR -138; BP -90/44; SPo2 -not picking up; RR -28 Temp -100.1 F
Week 3: Clinical Setting: 92 y F with HTN, remote breast cancer, Parkinson’s presents with generalized weakness and bilateral leg swelling.
Week 4: Clinical Setting: 68 y F who presents with agitation, with a reported intentional benzodiazepine overdose. HR - 70
BP - 175/110 RR - 20 SpO2 - 97% Temp - 99.2 F
Week 5: Clinical Setting: 44 y M with a history of alcohol use disorder presents with confusion. HR - 78, BP - 155/64 RR - 14 SpO2 - 97% Temp - 98.5
Week 6: Clinical Setting: 55 y M with CHF (EF 30-35%), HTN, schizophrenia who presents after he had a pre-syncopal episode.HR - 78, BP - 148/96, RR - 16, SpO2 - 95% RA Temp - 98.4 F
Week 7: Clinical Setting: 77 y F with HTN, Parkinson’s, DMII who presents with shortness of breath for 2 days, worsening today. HR - 95, BP - 165/87, RR - 18, SpO2 - 93%, Temp - 99.1 F
Week 8: Clinical Setting: 64 y M with history of CAD, HTN, mild aortic stenosis who presents with lightheadedness.
Week 9: Clinical Setting: Clinical Setting: 74 y F with HTN, HLD, DMII, COPD who presents with chest pain.
Week 10: Clinical Setting: 71 y M with history of heavy smoking, but otherwise does not see a doctor or have any known medical problems, presents with tachycardia, and a month of fatigue with exertional dyspnea.
HR - 136
BP - 158/95
RR - 22
SpO2 - 93% on AR Temp - 99.1 F
Week 11: Clinical Setting: 70 y M with VF arrest, s/p ROSC in the field. Unresponsive.
HR - 62
BP - 98/55
RR - 22
SpO2 - 98% on NRB Temp - 96.9 F
Week 12: Clinical Setting: 50 y M with CAD s/p CABG, COPD, cirrhosis who presents from his primary care doctor with an abnormal EKG, palpitations.
HR - 160
BP - 125/66
RR - 20
SpO2 - 93% on RA Temp - 97.8 F
Week 13: 62-year-old female with no significant PMHx presents to the emergency department with syncope. She was walking her dog when she suddenly syncopized. She denies any prodromal symptoms or associated chest pain, palpitations, or shortness of breath. She denies any recent sick symptoms or decreased PO intake. She denies any similar episodes in the past.
Week 14: 56-year-old male with PMHx HTN, HLD, T2DM, COPD presents to the emergency department with chest pain. Patient reports he was out mowing his lawn when he suddenly developed mid-sternal chest pressure with some associated diaphoresis. He denies any radiation to his arms or neck. He endorses some mild associated shortness of breath. He called 911 and EMS loaded him with ASA 324 mg en route to the hospital. He still complains of ongoing chest pain during your evaluation.
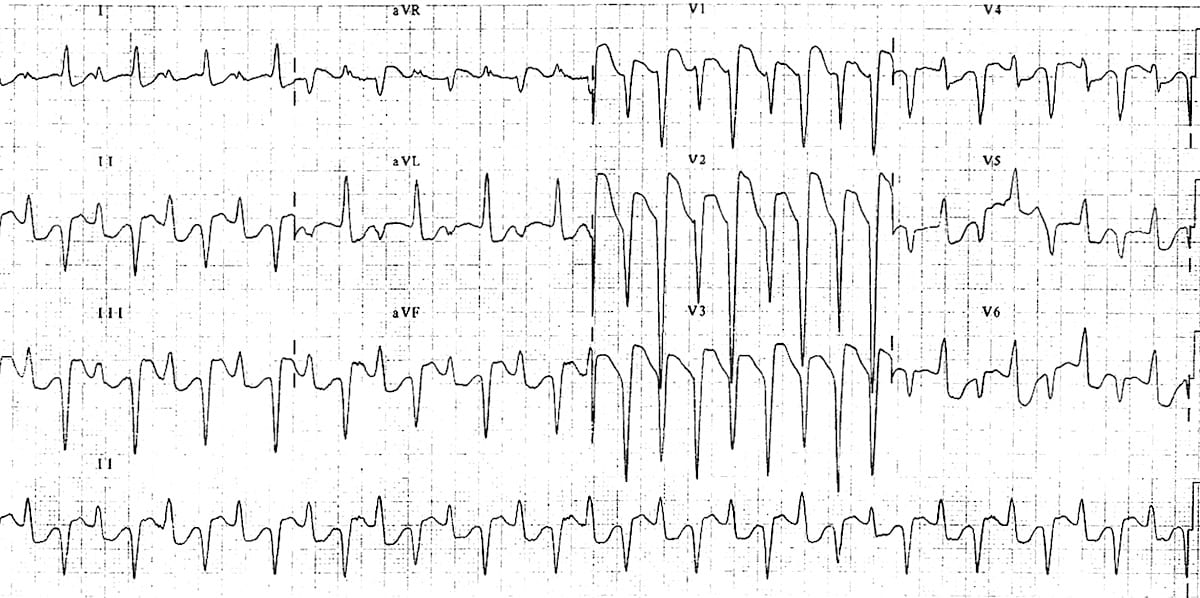
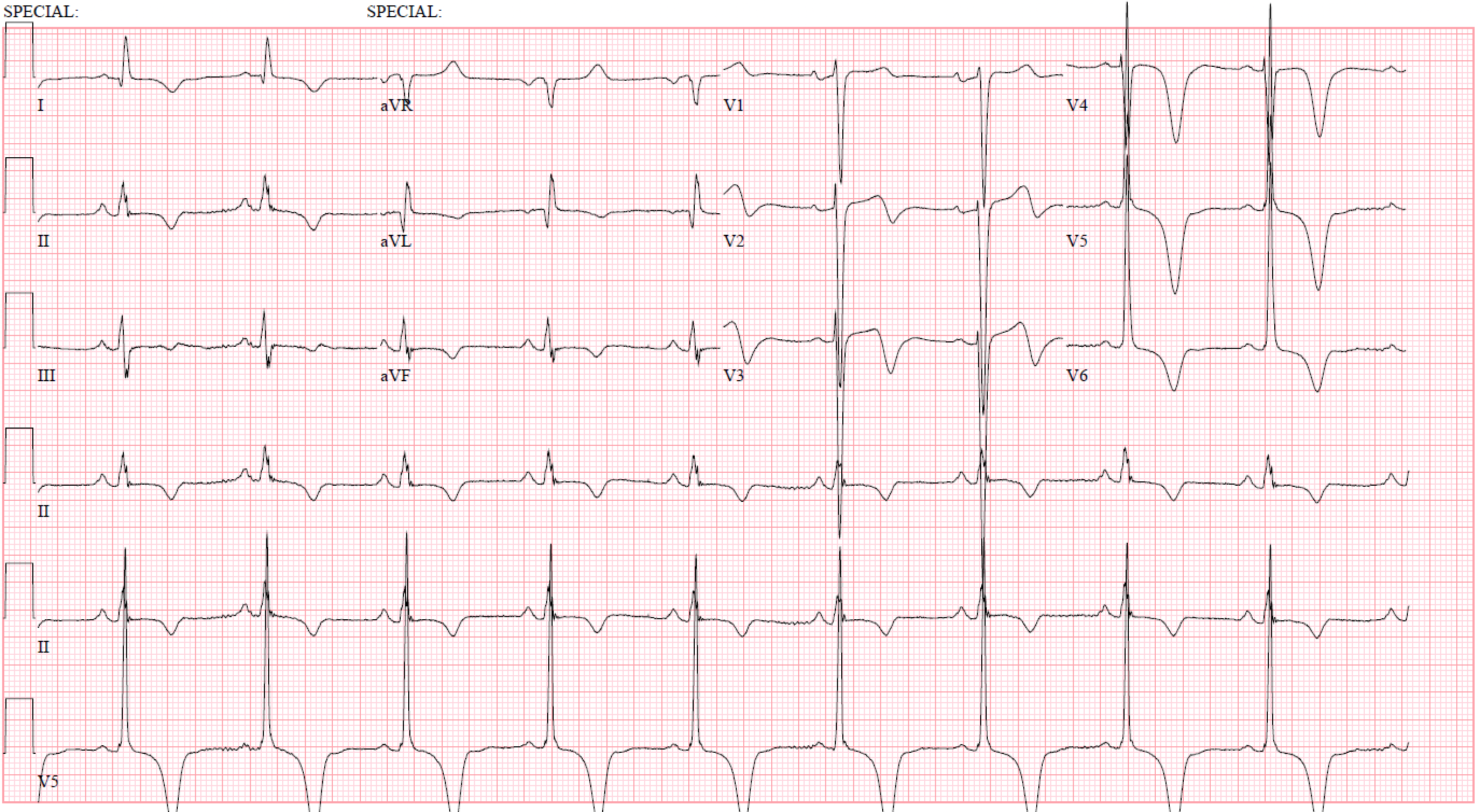
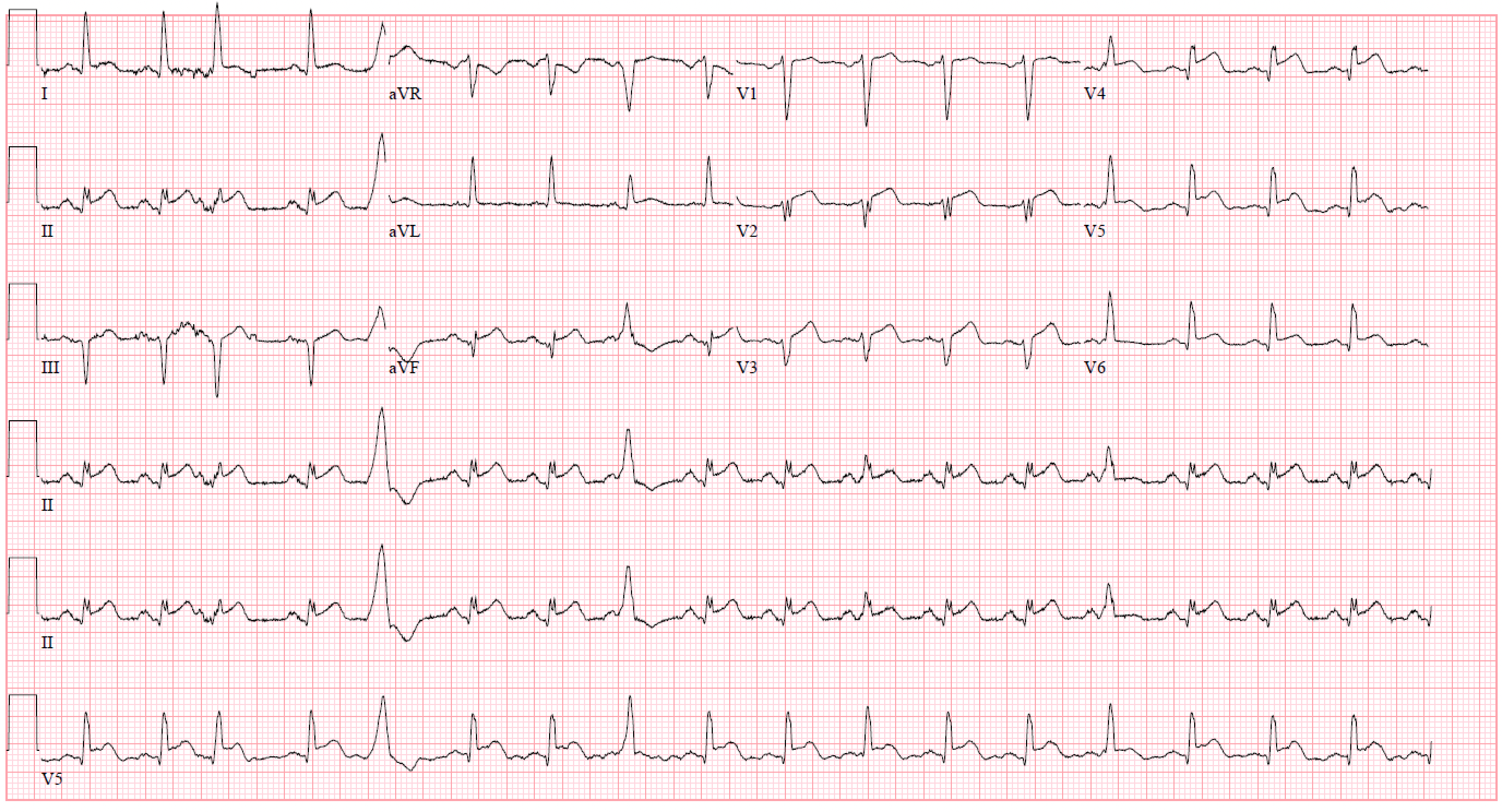
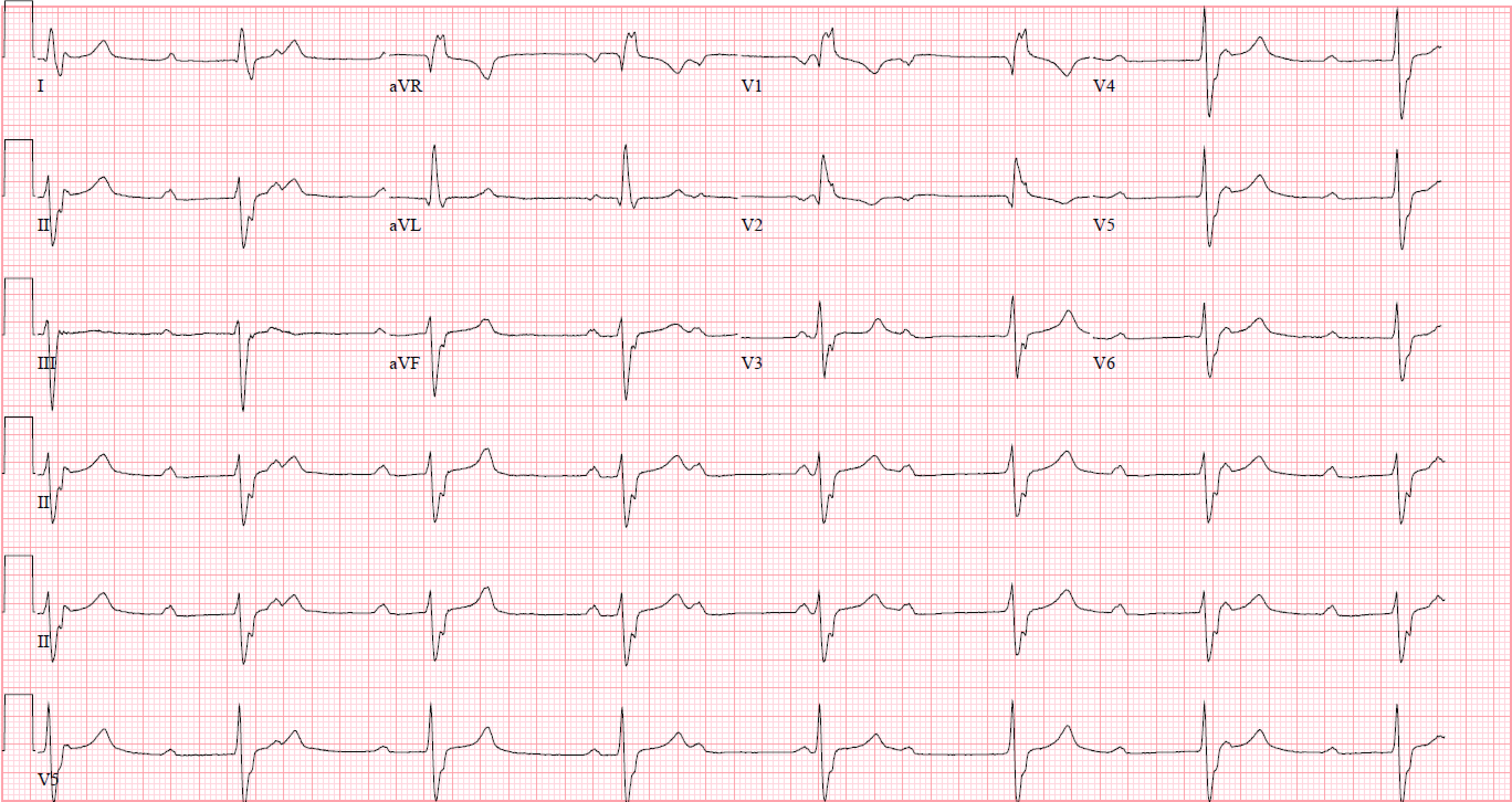
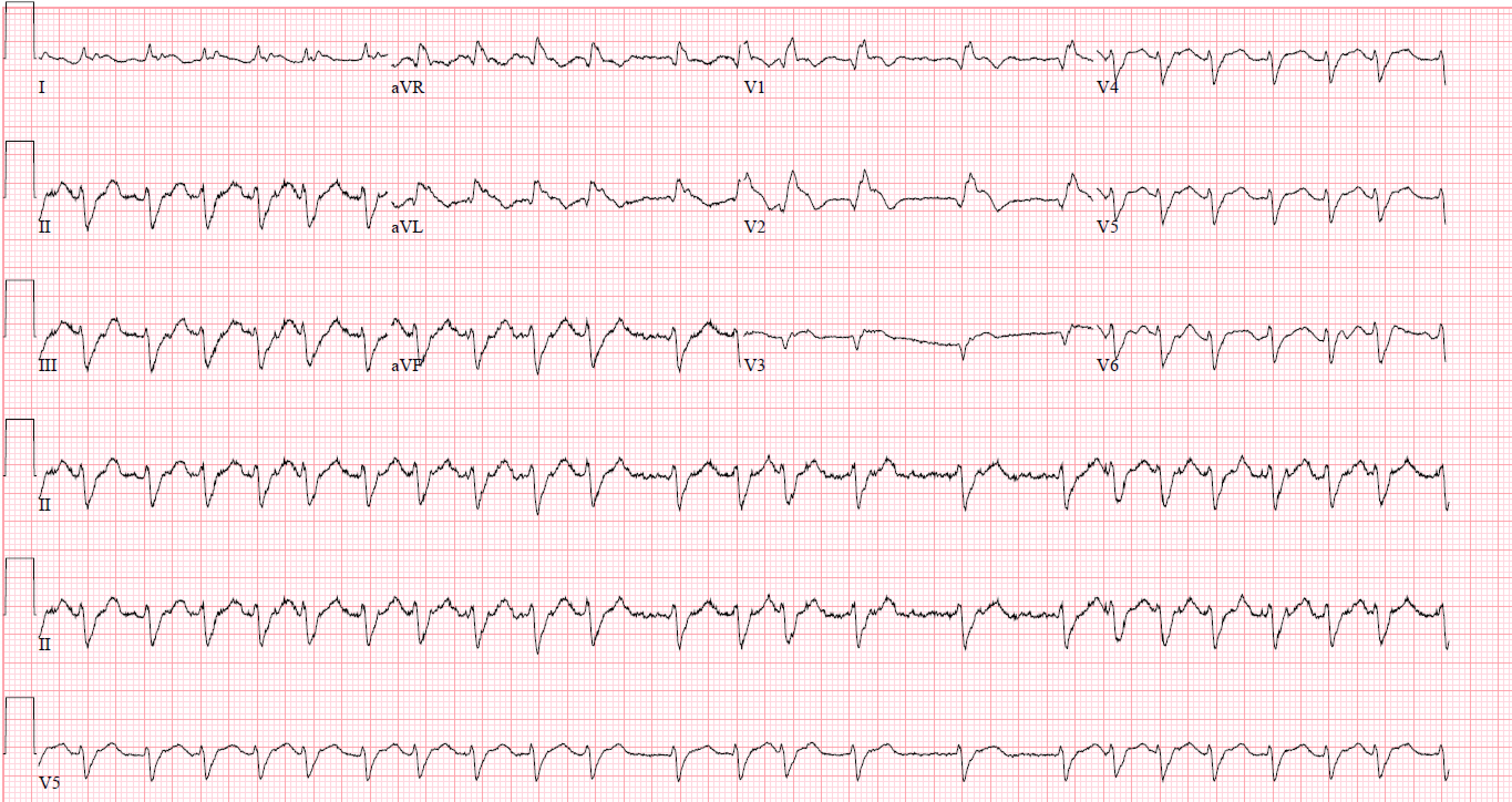
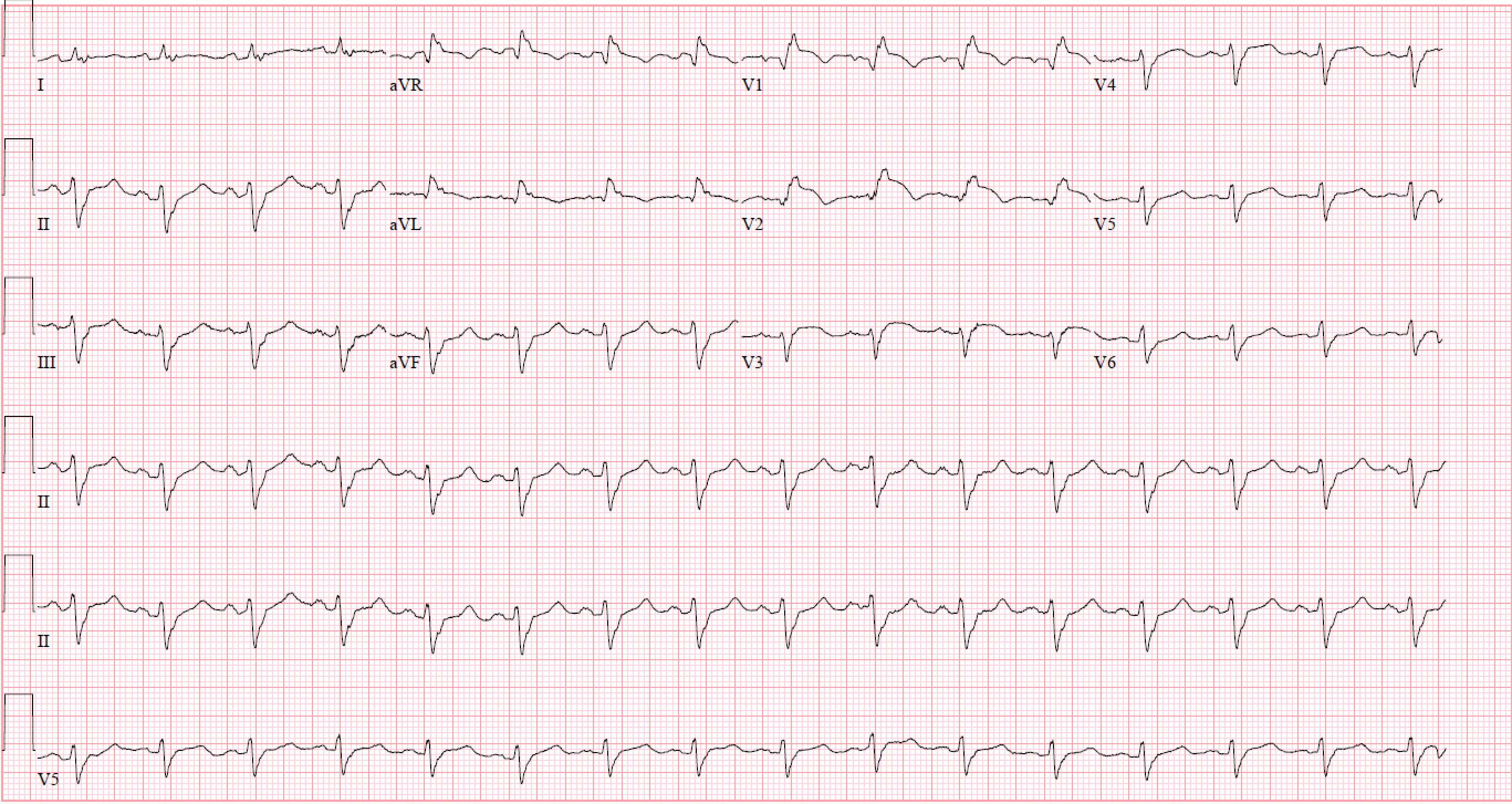
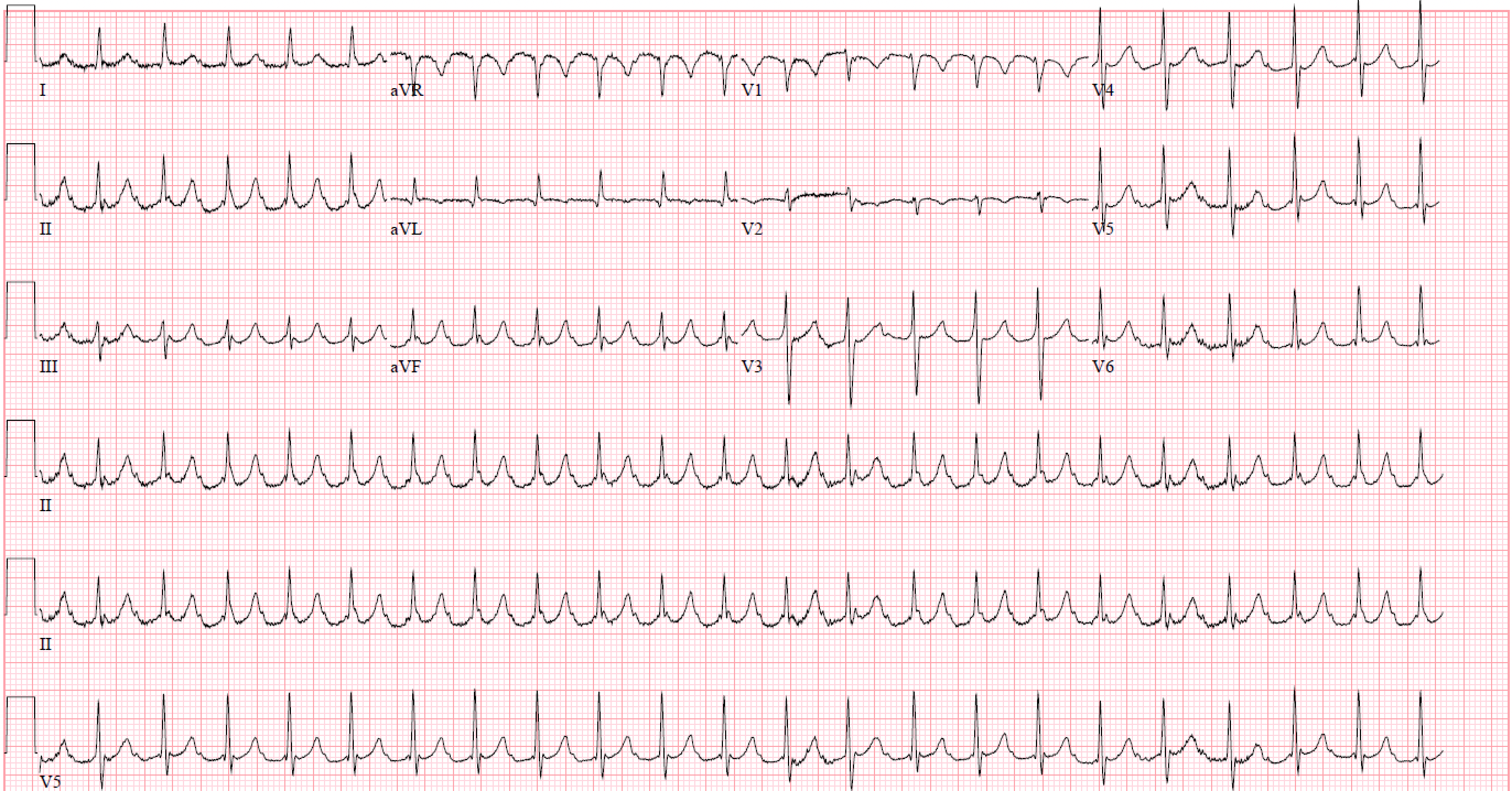
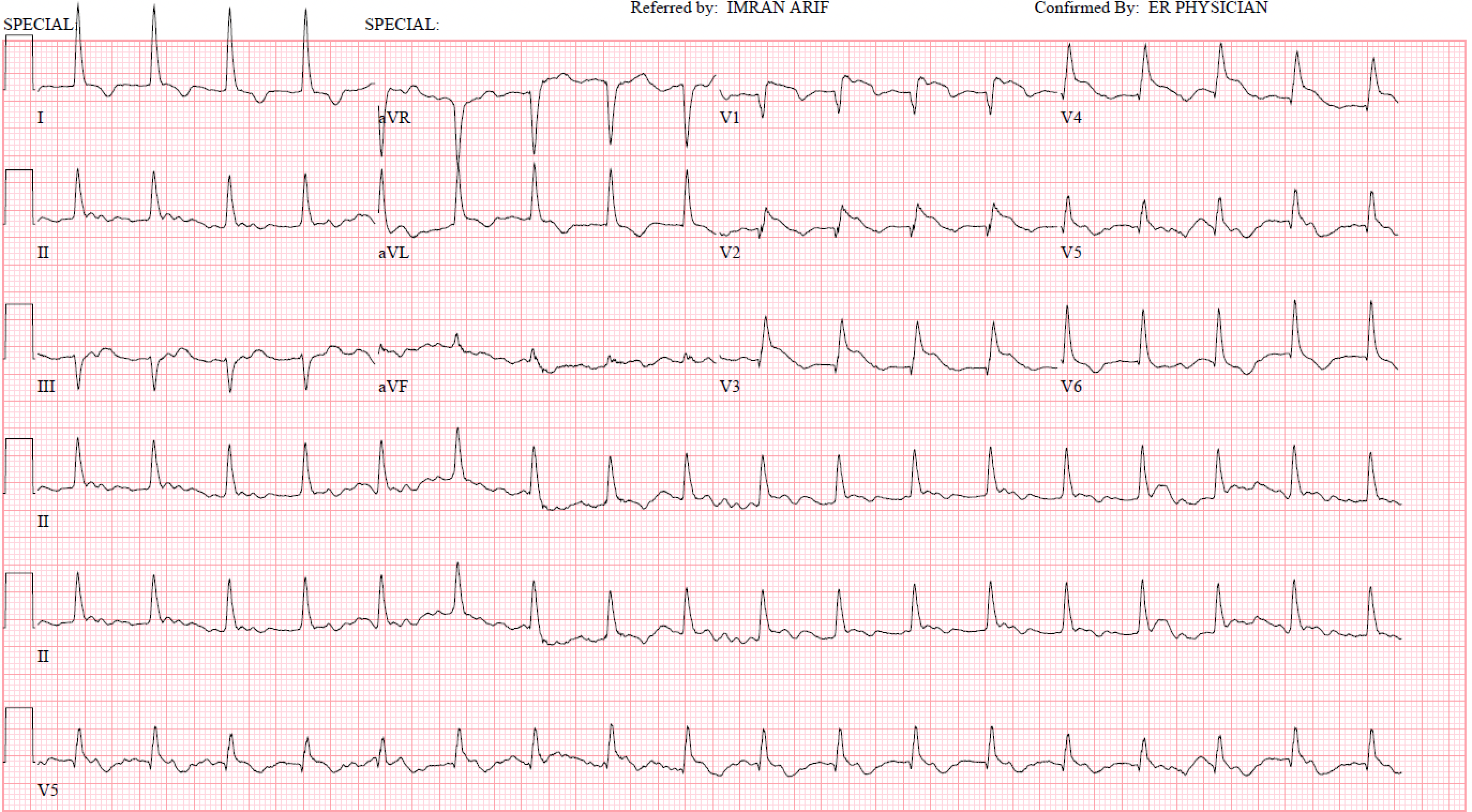
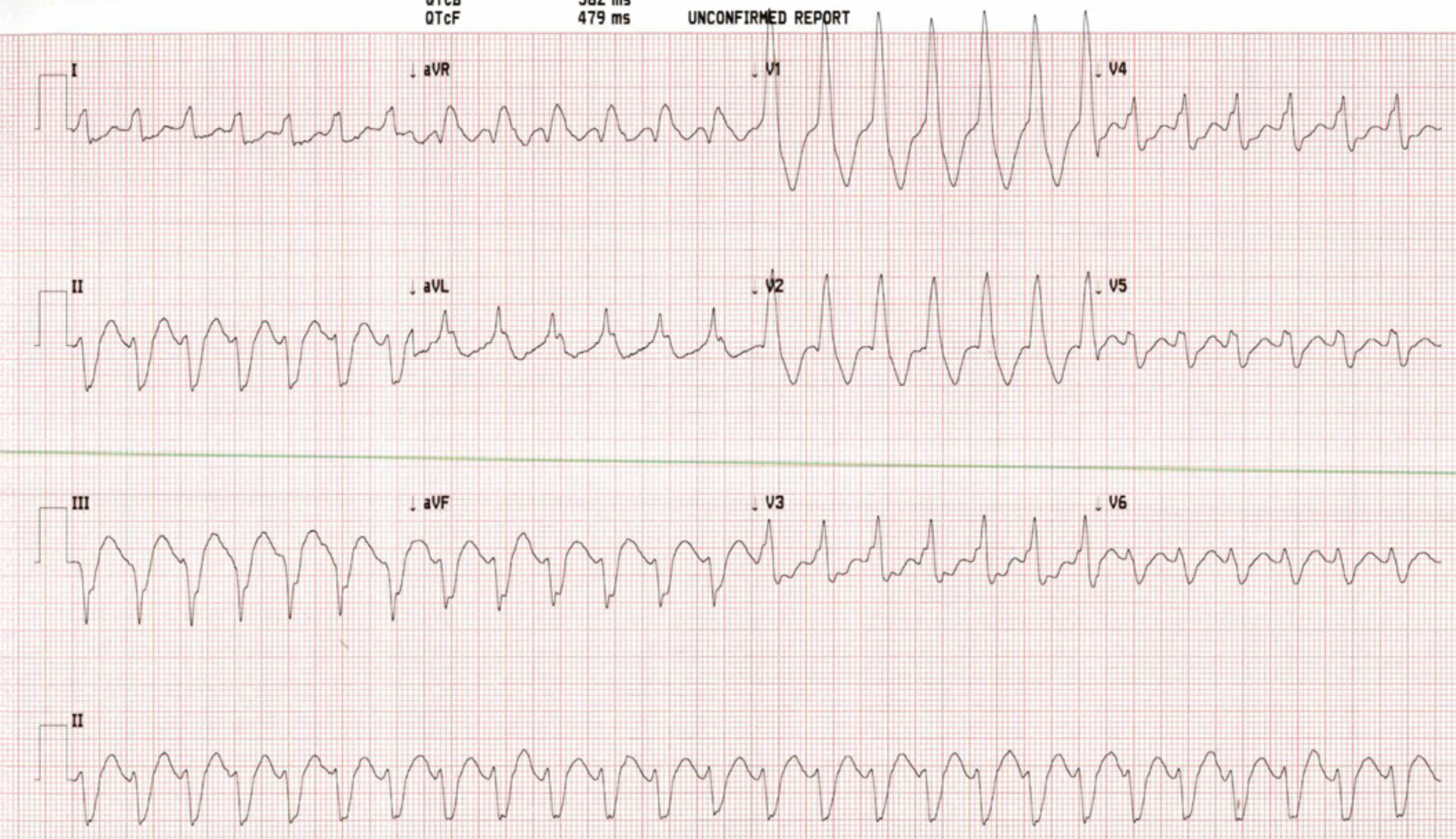
Week 15: 26 y/o M without significant medical history who presents for sudden onset palpitations and shortness of breath.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}