The Anatomy of Femoral Vascular Access
/Prior to the widespread availability of point-of-care ultrasonography, invasive medical procedures were performed by the “landmark method”. Landmark methods are based on surface anatomy, palpation, and sometimes trigonometry, and are fraught with the potential for error. Complications, while unquantified in the misty past, were likely much more common than in the current era of readily available bedside imaging. Vascular access procedures are inarguably safer and more successful when guided by sonography, but interpretation of ultrasound images still requires an understanding of both surface and deeper anatomy to relate the two-dimensional screen image to three-dimensional reality. Further, there are circumstances where either the urgency of the resuscitation, or compromised access to the patient, requires that vascular access be obtained using landmarks rather than real-time imaging. In such cases a detailed understanding of regional anatomy is critical to maximize procedural success and minimize complications.
Femoral Triangle
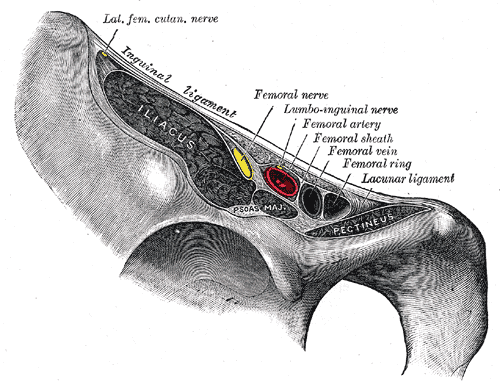
Figure 1 - Anatomy of the Femoral Triangle. Gray's Anatomy Plate 545 from Wikimedia Commons
The relevant anatomy for femoral arterial or venous access is that of the femoral triangle (See Figure 1), a subfascial space in the anterior thigh with the following boundaries:
- Superior - Inguinal ligament.
- Lateral – Medial border of the sartorius muscle.
- Medial – Lateral border of the adductor longus muscle.
- Superficial – Skin, subcutaneous fat, superficial fascia, fascia lata.
- Deep – Muscular fascia of the pectineus, psoas and iliacus muscles
The skin of the thigh is relatively thin and is mobile due to a loose connection with the underlying fascia. The subcutaneous layer contains a variable amount of fat superficially, and is delimited on its deeper portion by a fibrous layer. The superficial inguinal lymph nodes and cutaneous nerves and subcutaneous vessels of the upper thigh (i.e., the great saphenous vein) lie between the fatty and fibrous layers. The mobility of the skin overlying the femoral triangle is significant: A surface landmark can shift several centimeters relative to deeper structures if traction (including gravity) or pressure is applied to the skin, or if the thigh moves after identification of surface landmarks but before insertion of the needle. The compartment between the fascia lata and the underlying muscular fascia of the iliacus, psoas and pectineus muscles forms the subfascial space that contains the femoral vessels.
Figure 2. Inguinal Ligament. Gray's Anatomy Plate 546 from Wikimedia Commons
The inguinal ligament is the inferior edge of the aponeurosis of the external abdominal oblique muscle. It attaches to the anterior superior iliac spine and the pubic tubercle and separates the anterior abdominal wall from the thigh (see Figure 2). It is the critical surface landmark for femoral vascular access, marking the transition between the femoral vessels (below) and the external iliac vessels (above). The inguinal ligament is often palpable in lean individuals. When the ligament cannot be palpated, its surface course can be accurately estimated by a straight line between the anterior superior iliac spine and the pubic tubercle. An overlying surface landmark, the inguinal crease, is notoriously unreliable as a landmark for the ligament; it sags and is well inferior to the ligament in > 70% of patients (1), and lies a mean distance of 1.8 cm cephalad to the bifurcation of the CFA (2).
The familiar mnemonic NAVL (Nerve, Artery, Vein, Lymphatics) describes the sequence of neurovascular structures within the femoral triangle from lateral to medial.
Femoral Artery
The common femoral artery (CFA) is the continuation of the external iliac artery as it passes beneath the inguinal ligament. It is variable in length, 2 cm to 6 cm in a Romanian study (3), and an average of 7.5 cm in an American study (2). It varies in diameter from 6 mm to 10 mm depending on body habitus and volume status (4). The artery enters the femoral triangle near the midpoint of a line from the anterior superior iliac spine to the pubic tubercle. It terminates at its bifurcation into the superficial femoral artery (SFA) and deep (profunda femoris) femoral artery (DFA) (see Figure 3). Distal to this bifurcation, the arterial walls are significantly thinner than in the CFA and the vessels are not compressible against an underlying bony structure. Hemorrhage and pseudoaneurysm formation are much more common when arteriotomy occurs at the level of the SFA (5). The inferior epigastric artery is the last branch off of the external iliac artery before it passes beneath the inguinal ligament (see Figure 3). This artery can be palpated in the inguinal canal of males, and is visible on sonography in both genders. It is a significant landmark; retroperitoneal hemorrhage occurs almost exclusively when arteriotomy occurs proximate to the origin of this branch (6, 7) where the posterior wall of the artery lies above the pelvic brim and within the retroperitoneal space (see Figure 4).
Figure 3 - Branches of the Iliac and Common Femoral Arteries
Figure 4 - Iliac Artery and Vein. Gray's Anatomy Plate 547 from Wikimedia Commons
The CFA overlies the medial portion of the femoral head in the middle of its course. In this area it is palpable when compressed against the underlying bone. This portion of the vessel, approximately 2 - 3 cm distal from the inguinal ligament, is the safest site for femoral puncture (see Figure 3 above). Often, this portion of the artery is identifiable as the site of maximal femoral pulse (8).

Figure 5 - Equilateral Triangle
Keep in mind that the arterial puncture and the needle entry points in the skin are not at the same level. When the needle is passed at a 45 degree angle cephalad, the skin puncture should occur distal to the desired arteriotomy site at a distance equal to the depth of the uncompressed vessel (45-45-90 triangle rule) (see Figure 5). When bedside sonography is available, the vessel depth can be measure directly. When landmark methods are used, this distance must be estimated by the depth of compression required to palpate a strong pulse.
Femoral Vein
Figure 6 - Anatomy of the Femoral Vein. Gray's Anatomy Plate 549 from Wikimedia Commons
The common femoral vein (CFV) lies just medial to the CFA in the proximal part of the femoral triangle, but spirals to a position posterior to the artery as they pass distally to enter the adductor canal. The CFV is formed in the femoral triangle by the juncture of the superficial femoral vein (SFV) and the deep femoral vein (DFV). This juncture is variable, occurring between 5 cm and 11 cm distal to the inguinal ligament (avg. = 8 cm) (9). The CFV is also variable in diameter depending on the body habitus and volume status of the patient. It receives various tributaries, including the greater saphenous vein, prior to passing deep to the inguinal ligament and becoming the external iliac vein (see Figure 6). The greater saphenous vein is easily visible on ultrasound, entering the CFV on its anteromedial aspect. The CFV typically contains two valves, one just proximal to the juncture of the SVF and DFV and one as it transitions into the external iliac vein.
The safest site for puncture of the CFV is immediately proximal to the saphenous intake. Venipuncture below this level may inadvertently enter the greater saphenous vein resulting in blood return but difficulty passing a guidewire, or puncture of the CFA as the vein spirals behind it in more caudal portions of the femoral triangle. In the absence of bedside sonography, a point two finger-breadths below and one finger-breadth medial to the junction of the middle and medial thirds of a line from the anterior superior iliac spine to the pubic symphysis will approximate the proper venous puncture site. If the femoral pulse is readily palpable, the vein will generally be encountered 1 cm medial to the femoral pulse. The skin puncture site should be slightly caudal to the desired venous puncture site by the same logic mentioned above for CFA puncture.
References
- Cox, N. (2008) Managing the femoral artery in coronary angiography. Heart Lung Circ. 17 Suppl 4:S65-9. doi: 10.1016/j.hlc.2008.08.007.
- Garrett PD, Eckart RE, Bauch TD, Thompson CM, Stajduhar KC. (2005) Fluoroscopic localization of the femoral head as a landmark for common femoral artery cannulation. Catheter Cardiovasc Interv. 65(2):205-7. PubMed PMID:15900552.
- Crisan, S. (2012) Ultrasound examination of the femoral and popliteal arteries. Medical Ultrasonography. 14(1): 74-77.
Sandgren, Thomas et al. (1999) The diameter of the common femoral artery in healthy human: Influence of sex, age, and body size. Journal of Vascular Surgery. 29(3):503-510.
Cheri Davis, Sharon Vanriper, Jennifer Longstreet, Mauro Moscucci. (1997) Vascular complications of coronary interventions. Heart & Lung: The Journal of Acute and Critical Care. 26(2):118-127. https://doi.org/10.1016/S0147-9563(97)90071-6.
Sherev, D. A., Shaw, R. E. and Brent, B. N. (2005). Angiographic predictors of femoral access site complications: Implication for planned percutaneous coronary intervention. Cathet. Cardiovasc. Intervent. 65: 196–202. doi:10.1002/ccd.20354
Ellis, S. G., Bhatt, D., Kapadia, S., Lee, D., Yen, M. and Whitlow, P. L. (2006). Correlates and outcomes of retroperitoneal hemorrhage complicating percutaneous coronary intervention. Cathet. Cardiovasc. Intervent., 67: 541–545. doi:10.1002/ccd.20671
D. Grier and G. Hartnell. (1990) Percutaneous femoral artery puncture: practice and anatomy. The British Journal of Radiology. 63(752): 602-604.
Edwards E., Robuck J. (1947) Applied anatomy of the femoral vein and its tributaries. Surg Gynecol Obstet. 85(5):547-57. PubMed PMID: 20266767.




{kind=link}
{kind=link}
{kind=link}
{kind=link}