Cricothyrotomy
Make the Decision to Cut
“The most important complication for the patient in the context of surgical airway management is when delayed decision making after initial intubation failure leads to prolonged ineffective intubation attempts that result in hypoxic injury” (1)

There are a number of factors that can make the performance of a cricothryotomy particularly challenging - lack of familiarity with the procedure, poor landmarks, or any of the known predictors of difficult via the SHORT acronym. But the cognitive barriers to performing this procedure dwarf any technical barriers.
It is critical that when a can't intubate, can't ventilate scenario arises, the leader of the resuscitation verbalizes the situation and verbalizes the need to perform a cricothyrotomy. (See this video by Yen Chow, MD for a good example of clear communication during this situation) When you are visualizing yourself in this situation, performing this procedure and when you are practicing in the simulation center, don't forget to practice your communication.
It is also important to be prepared to do this procedure on each and every airway. When verbalizing the plan for laryngoscopy, verbalize your plan for cricothyrotomy. Have the kit out. If you feel there is a significant chance the patient will need to have a cricothyrotomy performed, go ahead and prep the neck, locate and mark your landmarks, open up the kit, maybe even inject some lidocaine with epinephrine. (See the EMCrit post on CricCon for more discussion of this).
Prepping the Patient and Prepping yourself
Prepping the Patient's Neck
Should use either chlorhexidine or betadine to clean the skin in preparation for the procedure
Anesthetize using 1% lidocaine w/ Epinephrine
Preparing Yourself
Put a face shield on as this procedure can be quite bloody with a high probability of blood spray once you enter the airway (see the video of a cricothyrotomy performed on a real patient as evidence)
Calm yourself - tactical breathing to decrease your heart rate and your stress as you get ready to perform the procedure
Identify the Relevant Anatomy & Give the Larynx a Handshake
Screencast of the anatomy involved in a cricothyroidotomy. This isn't going to tell you how to do it, there's smarter people to do that! by Andy Neil, MD of the EmergencyMedicineIreland Blog. https://vimeo.com/37340167
A thorough understanding of the relevant anatomy, and the techniques for identifying the cricothyroid membrane (CTM), is absolutely necessary for successful performance of this procedure. Do NOT underestimate how challenging identification of the anatomy can be. A recent study by Bair and Chima (2015) found that general palpation of the anatomy led to accurate identification of the CTM only 62% of the time.
The cricothyroid membrane is bounded superiorly by the thyroid cartilage and inferiorly by the cricoid cartilage. It is more easily palpated in thin male patients, 1 fingerbreadth below the laryngeal prominence. In obese patients (more soft tissue) and in female patients (less prominent thyroid notch), it may be more difficult to identify. Check out the embedded video by Andy Neil, MD of EmergencyMedicineIreland.com for some more discussion of the anatomy.
Dr. Rich Levitan describes a method of identification and stabilization called the “laryngeal handshake” in this article. As seen in the photo below, the thumb and index finger of the dominant hand is used to first identify the hyoid bone (pic 1). The index finger is brought to midline (to identify the thyroid prominence in men) while the thumb and middle finger slide down the neck to identify the thyroid lamina (pic 2). Nearing the bottom of the thyroid cartilage the cricoid cartilage is appreciated (pic 3) and the index finger is used to identify the cricothyroid membrane (pic 4). Once identified the process is repeated using the non-dominant hand which will stabilize the laryngeal “cartilaginous cage” during the procedure.
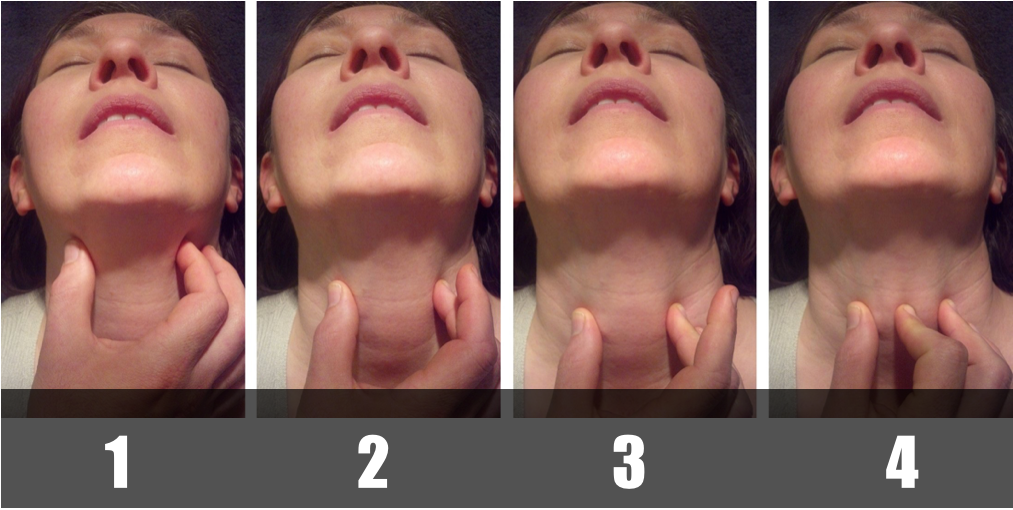
Adapted from Levitan, R. Laryngeal Handshake - Hyoid - Thyroid - Cricoid > Cricothyroid membrane http://www.airwaycam.com/airway-images-drawings/?gmedia_gallery_id=2&gmedia_gallery_share=74
Making the Cut, Dilating, and Passing the Tube
(As a recap from above) the non-dominant hand is stabilizing the laryngeal cartilaginous cage and the non-dominant index finger is able to palpate the cricothyroid membrane.

Levitan, R. Stabilizing scalpel hand on sternum during cricothyrotomy http://www.airwaycam.com/airway-images-drawings/?gmedia_gallery_id=2&gmedia_gallery_share=76
The dominant hand holds the #10 or #20 blade using the sternum of the patient to stabilize the hand during the procedure.
A 2 to 3-cm vertical skin incision is made in the midline (some providers advocate for a slightly more generous incision of 3 finger breadths to get maximum exposure)
The cricothyroid membrane is again identified using the index finger of the non-dominant hand.
A horizontal incision is made into the lower half of the cricothyroid membrane. The blade of the knife is flipped and the incision is extended in the opposite direction.
The tracheal hook is inserted in the transverse plane and then rotated cephalad to grab the inferior thyroid cartilage.
The incision in the cricothyroid membrane can now be dilated with a Trousseau dilator or a finger.
A bougie is passed into the trachea helping confirm placement by feeling the “washboarding” of the tracheal rings as well as by depth of insertion (ref). The 6-0 ET tube can then be passed over the bougie into the trachea.
Inflate the cuff on the endotracheal tube and confirm via EtCO2 and auscultation as per usual.
Lets Take A Look at the Procedure in Action


Requires Institutional Access
The bougie can make an open cric much easier. Here is airway master Darren Braude, MD demonstrating this technique. See more bougie magic at http://airway911.com
This video shows you, first person, what it is like to perform a cricothyrotomy with a bougie. Performed by Bill Hinckley, MD
The Sharp End Crew - http://www.thesharpend.org/eeacc-7-surgical-airways/
Additional Excellent #FOAMed Resources
References
Vissers, R. & Bair, A. Surgical Airway Techniques. Manual of Emergency Airway Management. 3rd Edition. Chapter 16. pp 207.
Chow, Yen. Scalpel Finger Bougie Cric Trainer. https://www.youtube.com/watch?v=jWYo8p0cRU8. Accessed 8/10/2015
Bair, A & Chima, R. (2015) The Inaccuracy of Using Landmark Techniques for Cricothyroid Membrane Identification: A Comparison of Three Techniques. Academic Emergency Medicine. 22(8):908-14. doi: 10.1111/acem.12732
Weingart, S. EMCrit Wee – Bougie Prepass and CricCon for Difficult Airway. http://emcrit.org/wee/bougie-prepass-and-criccon/. July 4, 2012. Accessed 8/10/2015
Neil, Andy. Anatomy for Emergency Medicine #7 Cricothyrotomy. https://vimeo.com/37340167. Accessed 8/10/2015.





{kind=link}