US - Saphenous vein cannulation: Ultrasound of the Month
/Case
The patient is a middle agred, obese female with history of renal transplant one year ago presenting with abdominal pain. Her pain is poorly localized, has been present for the past day, and is associated with several episodes of non-bloody emesis and subjective fevers. She reports no urinary symptoms or changes in bowel habits. On exam she is afebrile and hemodynamically stable in no acute respiratory distress. She appears uncomfortable and has generalized abdominal tenderness with no rebound or guarding.
You return to your station and place your orders for workup, already mentally shifting to the next task, but several minutes later you are approached by your nurse after several unsuccessful attempts at IV access. Confident in your skill at ultrasound-guided peripheral access you bring the machine and supplies into the patient’s room, however after two tries at a deep brachial vein in her left arm you are thwarted by her deep, sclerotic, and fragile veins. You look to the right arm for redemption, but are dismayed to find a dialysis graft that immediately dashes your hopes.
What will be your next move? A central line perhaps? As you contemplate your options the trauma pager sounds its cry from your waist warning you of the expected arrival of a sick trauma patient in 10 minutes. The patient in front of you needs access to begin her diagnostic evaluation and therapy ideally before you are drawn away for a potentially prolonged resuscitation elsewhere.
It then occurs to you that in times past a saphenous vein cutdown was a fairly standard technique for vascular access in a challenging patient. Before you decide to break out a 10-blade, remember that you are equipped with an ultrasound machine and an IV catheter...
preparation

probe and angiocath positioning for cannulation. Also you may consider in-plane technique.
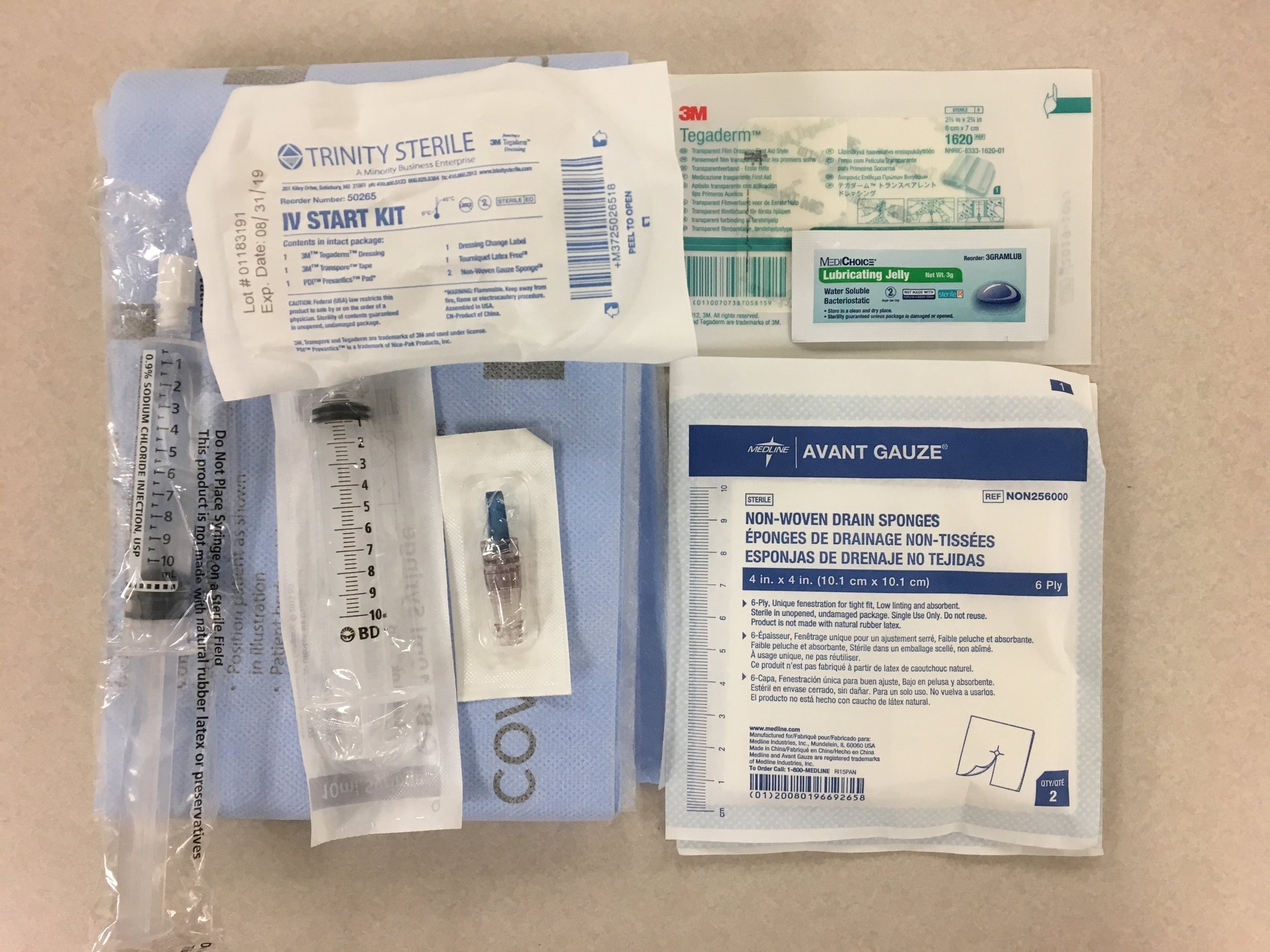
Supplies needed including an extra tegaderm to cover the US probe, and 1.88" angiocath
Cannulation in the transverse Plane

Cannulation in the Longitudinal Plane

Discussion
Ultrasound guidance has been shown to increase the likelihood of successful venous cannulation in patients with difficult access (1) and to improve speed, result in fewer complications, and increase patient satisfaction (2) when compared with traditional blind techniques. A variety of patient factors can make cannulation of upper extremity veins difficult including obesity, IV drug use, and repeated access due to chronic illnesses. As we have moved away from performing saphenous cutdowns we have become more prone to using intraossesous or central venous access, however these lines are associated with higher rates of complications including pain, extravasation, compartment syndrome, and infections (3,4).
The saphenous vein presents a viable alternative option when the veins of the upper extremity are difficult to access. For the purposes of peripheral cannulation, the preferred site should be just above the medial malleolus as the vein is at its widest and most superficial when compared to sites at the midcalf and below the knee (5). Supplies for the procedure are depicted in the photograph and are the same as those used for the upper extremity, although providers accustomed to using the 2.5” IV catheter for deep brachial cannulation may find that using a shorter catheter preferable due to the more superficial location of the saphenous vein.
When selecting the site be sure to do a preliminary scan of both legs to identify the best target. In addition to applying a tourniquet, saphenous vein diameter is shown to increase with the patient placed in reverse trendelenburg position (5). Cannulation can be performed with the probe in either the transverse or long axis orientation depending on the operator’s level of experience and comfort.
This procedure should be performed clean, but need not be sterile, as is standard for peripheral access. Steps for performing the procedure are analogous to those for deep brachial access and are as follows:
Protect yourself with nitrile gloves. You may also consider placing an absorbent pad under the patient's leg to keep it clean.
Prep the area with an alcohol swab and cinch your tourniquet when your are ready to stick.
Use the sterile gel packets rather than the bottled variety.
In selecting the right IV catheter, keep in mind that the saphenous vein is much more superficial than a deep brachial vein. This means that the longer catheters that are often ideal for the upper extremity may be too long for this target.
Cannulate the vein in either the transverse or longitudinal plane as seen above.
For a transverse approach pierce the skin about 0.5cm from the probe at a 30-45 degree angle to the skin. The needle tip will appear as a bright white dot on your screen, and once you see this you should stop moving the needle. Sweep the probe forward until the dot disappears then stop moving the probe Advance the needle until you see the bright dot of the tip reappear, and continue to advance towards your target in a stepwise fashion until your needle is in the center of the vessel lumen and you have flash in the needle chamber.
For a longitudinal approach visualize the vessel with your probe. Unlike the deep brachial vein, the saphenous vein does not have a sister artery running along with it, so you should not need to use adjunctive techniques to differentiate the artery and vein. Pierce the skin with your needle at a 30-45 degree angle as close to the probe as you can manage. You may even tilt the probe forward slightly so that your entry point is actually a few millimeters under the edge. From here you should be able to watch your needle advance along its entire trajectory into the vessel.
Advance the catheter off of the needle and into the vessel then remove the needle and dispose of it in a sharps container.
Flush the line with a saline flush and cap the line with a blue cap.
Place your dressing and remove the tourniquet.
For a review of needle visualization for procedural guidance see here.
Although this procedure offers an alternative to intraosseous or central access in many patients, providers should use caution in patient selection and avoid those who may be prone to complications. Examples would be those with diabetes, peripheral vascular disease, and venous insufficiency.
Pearls
A significant subset of ED patients have factors leading to difficult peripheral access.
The saphenous vein should be considered as an alternative site for peripheral IV insertion if you are unable to cannulate the upper extremity.
Use caution in patient selection and avoid this procedure in patients who may be prone to complications.
Authored and Posted by Jared Ham, MD
Peer Reviewed by Lori Stolz, MD RDMS
References




