US - Gestational Sacn: Ultrasound of the Month
/The Case
G1P0 female with no prior history presents with lower abdominal cramping for approximately 24 hours. She was seen in the ED three days ago and had a positive pregnancy test. She was asymptomatic at that time without further pregnancy evaluation. Her last menstrual period was 8 weeks ago. The patient's vital signs are stable. On exam, she has mild lower abdominal tenderness on palpation but her abdomen is soft with no rebound or guarding. The rest of her exam is unremarkable. A bedside ultrasound is performed which reveals the following images:
+ What do you see on Ultrasound
These are transabdominal pelvic ultrasound views. The uterus is visible in the center of the images. Within the uterus is a gestational sac that is off to the side, aka eccentrically located. Some causes of an eccentric location are leiomyomas (fibroids - which this patient likely has, seen best on the transverse view), contractions while scanning, uterine anomalies, and even normal early pregnancies, which can appear eccentric. There are several tricky kinds of ectopic pregnancies in which the pregnancy may be mistaken as intrauterine but is truly not within the endometrial cavity. The terminology for these pregnancies can be really confusing...interstitial, cornual, angular, etc. Many people get these terms wrong, even obstetricians and radiologists. This leaves the rest of us perpetually confused. Below is a quick outline of the various terms:
Ectopic Pregnancy: Implantation of a gestation outside the endometrial cavity. Tubal, ovarian, abdominal, cervical, interstitial pregnancies are all ectopic pregnancies.
Interstitial Pregnancy: A gestational sac that implants within the interstitial portion of the Fallopian tube (the portion closest to the uterus). This is surrounded only by myometrium, no endometrium. These are typically considered nonviable (but a few really rare ones make it to viability). When ruptured, they can cause profuse bleeding because the uterus itself ruptures and during pregnancy it is a very, very vascular organ. Also, the gestation can grow much larger before rupture than a traditional tubal ectopic. If a patient is presenting with an interstitial pregnancy and it is unruptured, they can be imaged further (3D ultrasound, MRI). Some obstetricians may choose watchful waiting, but these pregnancies are usually terminated and many spontaneously abort.
Angular Pregnancy: A gestational sac that is implanted just medial to the utero-tubal junction, in the lateral angle of the uterine cavity. It may be surrounded by endometrium, but near the endometrial-myometrial border. It is not technically an ectopic pregnancy (considered intrauterine), but it is on the spectrum between normal and abnormal, with associated risks. These are potentially viable. There is a 38% rate of spontaneous or missed abortion and a 13% risk of rupture. In these pregnancies there is increased risk of preterm delivery, placental abruption, endometritis, and growth restriction. Obstetricians can discuss therapeutic abortion or watchful waiting with these patients.
Cornual Pregnancy: A gestational sac within the cornu (singular of cornua) of the uterus, in the superolateral region of the uterine/endometrial cavity where the Fallopian tube enters. Some people only use this term if the uterus is abnormal (bicornate, unicornate, etc), but some use it for normal uteruses with gestations that are interstitial or angular. It is a generally confusing term, perhaps to be avoided or otherwise qualified. Some pregnancies that are in the cornua are interstitial and therefore ectopic, some are not.
+ What are the Next Steps that Should be Performed in the ED?
If you visualize an eccentrically located pregnancy, what is the next step? First, when performing the scan, ensure that the entire uterus is captured in two orthogonal planes (meaning, two planes that are 90 degrees from one another; one longitudinal, one transverse). This can help better locate the pregnancy in the uterus. If it seems eccentrically placed, the next step is to measure the endomyometrial mantle. This is the section of the uterus (including the endometrium and myometrium) from the gestational sac to the external uterine wall. There is some debate about exactly what should be measured (endomyometrial versus myometrial mantle) and POC sonographers and OB sonographers tend to measure slightly different things. It is typically easier to measure the endomyometrial mantle because there are very clear lines to delineate where your measurement should be. You'll want to measure where you visualize the endomyometrial mantle is thinnest.
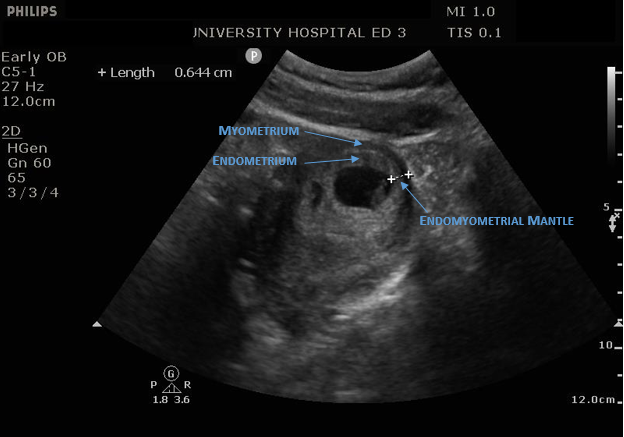
There is no clear consensus on the best cutoff measurement. 8mm is relatively conservative measurement and is typically used. If the measurement is less than 8mm, the patient should be going for a confirmatory study (if hemodynamically stable) and likely needs OB/Gyn consultation. The measurements for this patient were 9.7mm in the transverse view and 6.4mm in the longitudinal view (see image). Because of this, OB/Gyn was consulted. They agreed that the pregnancy was likely angular vs eccentrically located and elected for outpatient follow up.
Pearls:
Look for eccentrically placed gestational sacs
Always scan the entire uterus in two orthogonal planes
Look for an endomyometrial mantle measurement of 8mm
If less than that, get someone else involved, like our friendly OB/Gyns and radiologists




