Grand Rounds Recap 06.09.21
/
the art of emergency medicine WITH drs. lang, minges, d.thompson, adan, & stolz
This lecture serves to provide perspective on many of the ‘Cincinnati-isms’ that are common practice here and what, if any, data backs them up.
Benzodiazepine Pulses w/Dr. Lang
Recommendation: Lorazepam 0.5mg BID or TID x3 days for breakthrough seizure patients back to normal
Approach to breakthrough seizures (patient with known epilepsy who is back at neurologic baseline)
Precipitating factors - something that caused the seizure threshold to lower
Metabolic changes
Infection
Trauma
Alcohol use
Sleep
No precipitating factors
Usually sub-therapeutic dose
Treatment
Is the seizure different than normal (cluster of seizures, status, etc)? Yes → contact neurologist
Is the patient sick? Yes → treat precipitating illness, consider benzodiazepine pulse
AED level low? Yes → consider loading dose or oral dose in ED
Adjust dose for compliant individual
Therapeutic level? Yes → consult neurology
Few studies demonstrate giving a benzodiazepine pulse may quiet cluster seizures (small, completed by pharmaceutical companies)
Summary
Breakthrough seizures + back to baseline = careful history and exam
Check AED levels + load when possible
Benzodiazepine pulse
BUT potential helpful for those with clusters (3+ in 24 hours)
Also helpful for anyone with decreased seizure threshold (febrile illness)
Absorbable Sutures w/Dr. Minges
Absorbable suture
Pros: no need for removal? longer stability provided to wound?
Cons: most trials include return visits at around time of suture removal anyway, need to choose suture that dissolves when you want, theoretically more of a nidus for infection
Non-absorbable suture
Pros: need for removal (reevaluation isn’t always a bad idea), support to wound for as long as necessary
Cons: patient inconvenience, theoretically more of a nidus for infection
Data?
Mostly in kids and faces and post-op
Small studies with limitations
Absorbable sutures probably not inferior, though not definitively superior
Have a conversation with the patient to help you choose the right suture for the situation!
Ketofol w/Dr. Minges
Do not put them in the same syringe!
Ketamine 0.5mg/kg in ONE syringe
Propofol 0.5mg/kg in ONE syringe
Additional propofol PRN in a SEPARATE syringe
Only re-dose one medication - ketamine or propofol
Studies typically show ketamine is equivalent to ketofol in effect and side effects, but worth having in your armamentarium for the appropriate patient/situation
Ketamine for Severe Agitation w/Dr. D.Thompson
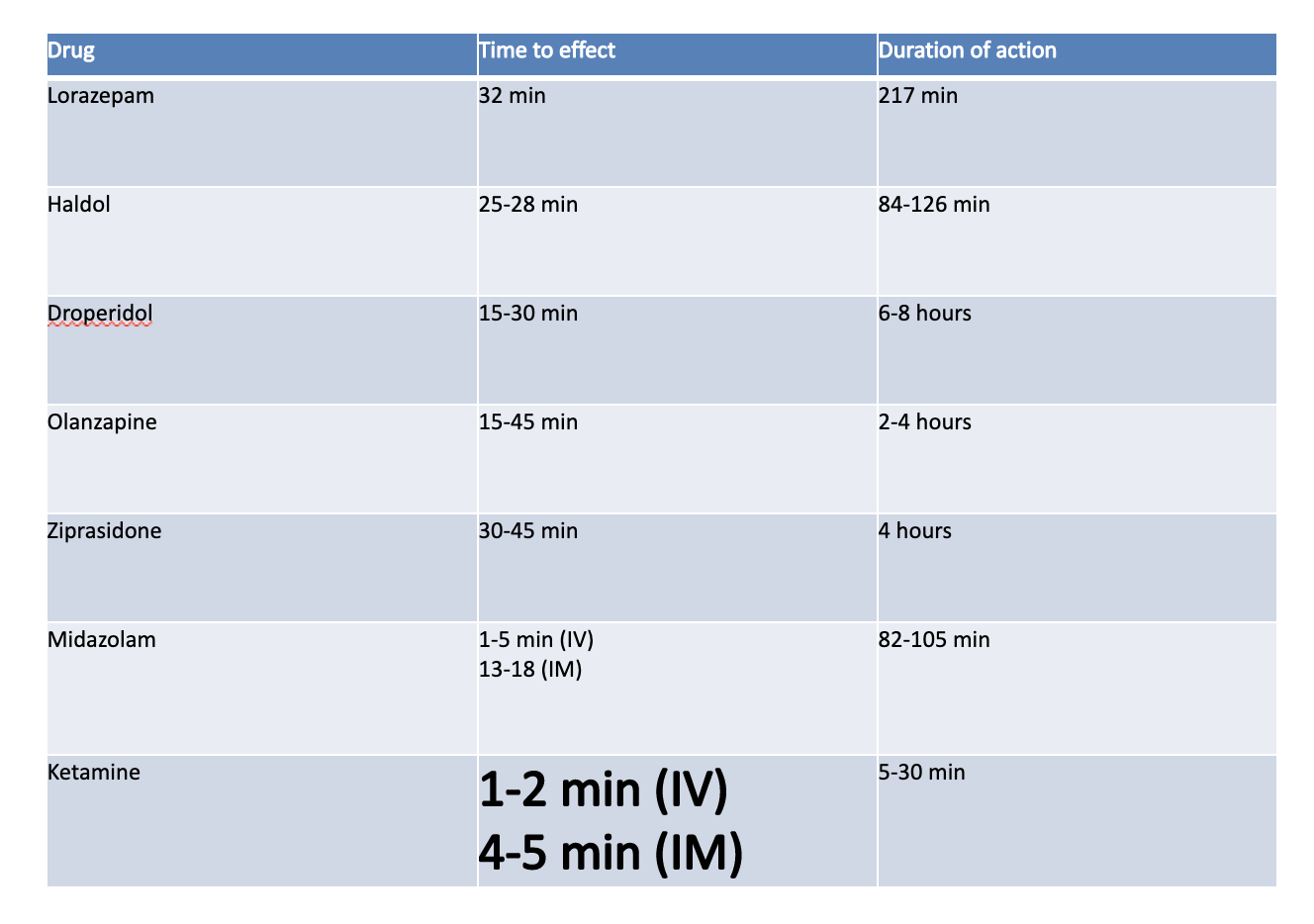
Consider this for the severely agitated, belligerent, and physically violent patient OR critically ill patient
High risk to patients and healthcare workers
Risk of other medications used in the agitated patient
Take time to take effect
Many cause respiratory depression
Many patients require repeat dosing
Ketamine benefits:
Rapid onset, near complete dissociation
Decreased respiratory depression compared to other agents (benzos)
Decreased need to re-dose to achieve behavioral control
Inclusion: severe agitation, violence, +/- head injuries, need for rapid control
Exclusion: mild agitation, anxiolysis, analgesia
Logistics
Ketamine 4-5mg/kg IM or 1-2mg/kg IV
Formulations: 10mg/ml, 50mg/ml, 100mg/ml
Communicate with nursing as patient will need 1:1 RN for 30-60min
Need full airway set up, ready to intubate
It’s procedural sedation - the procedure is safely taking care of the patient
A critical care procedure
Complete an appropriate sedation procedure note. Emergent consent will apply.
Adverse events: apnea, rigidity, partial dissociation, N/V, salivation, laryngospasm, psychiatric distress
Summary
Useful in selected cases when rapid control is necessary
Achieves rapid onset complete dissociation
+/- intubation
Treat as procedural sedation
Use high-concentration ketamine solution if giving IM to limit injected volume
Rhythm vs. Rate Control of Afib in ED w/Dr. D.Thompson
Single center (n=660) including ED patients with recent onset Afib [Stiell, 2010]
All got procainamide first with 58% cardioversion
243 electrically cardioverted with 91.7% success
Of those electrically cardioverted, 7% had hypotension with 8.6% had 7d relapse
No torsades, strokes, or deaths
Median ED LOS was 3.9h compared to 6.5h
Multi-center study (n=1091) including ED patients with recent onset Afib who got treated with rhythm control agents [Stiell, 2017]
9% admitted, 80% discharged in sinus rhythm
10% had adverse events within 30 days; no related deaths, 1 stroke
Patients who left the ED in sinus rhythm were much less likely to experience an adverse event
Effective, safe, and rapid protocol that can reduce inpatient admissions and expedite ED care
Consider electrical cardioversion in patients who are unstable, already therapeutically anticoagulated for at least 3 weeks, onset <12hr with no recent stroke, 12-48hr with CHADSVASC score 0-1, and cleared with TEE
“In patients presenting to the ED with recent-onset, symptomatic atrial fibrillation, a wait-and-see approach was noninferior to early cardioversion in achieving a return to sinus rhythm at 4 weeks” [Pluymaekers, 2019]
Summary
Selected patients with recent onset Afib may benefit from early rhythm control
Pay careful attention to stroke prevention
Requires shared decision making and appropriate documentation
NG Tubes for SBO w/Dr.Adan
The controversy: should we be placing NG tubes for all SBOs? Does it reduce length of stay, improve patient outcomes?
n=181 patients with SBO
Those with NG tube had longer LOS and higher rates of surgical bowel resection - may have confounding factors [Berman]
n=190
Complications associated with NG tube use include pneumonia (odds ratio 11.4), and any complication (odds ratio 19) - may have selection bias and other confounding factors [Fonseca]
Consider NG tube placement for SBO in the appropriate patient
RCTs demonstrate that midazolam administration prior to NG tube insertion decreases patient discomfort with the procedure
Alcohol Withdrawal Management w/Dr. Adan
Outpatient therapeutic considerations
Must be for patients who you do not think will go home and use alcohol
Benzos (valium, librium) - may need higher doses than you would otherwise prescribe for other pathologies
Gabapentin - can help with cravings and possible seizure prevention
Phenobarbital - loading dose of 10mg/kg (ideal body weight) and self-taper at home
Check hepatic panel for transaminases prior to administration
Trauma Pan Scan w/Dr. Stolz
Whole-body radiation exposure ~24.4mSv = 1 cancer deaths/100 patients scanned...very difficult to attribute to a single trauma pan scan
Con: cost, incidental findings, radiation
Pro: time to diagnosis, missed injuries
NNT scan between 17 and 32
Selective CT results in a 50% decrease in median injury severity score
REACT-2
>18yo and abnormal vitals or clinical suspicion of life-threatening injuries (n=1400)
No mortality difference (mortality 16% in both groups...very sick patients)
Radiation dose minimally lower in selective CT group
46% of selective CT patients ended up getting whole body CT
NEXUS Chest CT
Summer Penile Syndrome w/Dr. Stolz
Chigger bites to penis in children
A Cincinnati-ism - only two articles written about this are from Ohio
R1 CLINICAL KNOWLEDGE: hand infections WITH dr. gillespie
Evaluation:
Circumstances of the injury/development of symptoms, timeline
Systemic symptoms
Immune system factors: HIV? DM - last A1c?
Prior relevant infections (MRSA, HSV-1)
Occupation, hand dominance
Tetanus status
Exam:
Observation - wounds, swelling, natural resting position
This includes more proximally along the arm
Palpation - tenderness, crepitus, effusion
Motor
structural/tendon
Nerve motor function
Sensory
Vascular
Osteomyelitis
Presentation: Pain, swelling most commonly over the distal phalanx
Pathophysiology: Sequelae of other pathology, devascularization, contamination
Pathogens: Staph aureus and strep are most common
Less likely gram negative bacteria, anaerobes, atypical, fungal
Imaging
Surgical consultation
Treatment: antibiotics - parenteral: MRSA coverage + 3rd/4th generation cephalosporin
Septic arthritis
Presentation: Small joint of hand and wrist, with MCP/PIP most common
One small study reported a distribution of 25% wrist, 27% MCP, 20% PIP, 25% DIP, thumb DIP 2%
Pathophysiology: 65% associated with trauma
Pathogens: S. aureus (38% overall, MRSA 17%, MSSA 45%) most commonly isolated followed by group B strep
*sexually active patients with other clinical signs
Treatment: arthrotomy, debridement, antibiotics
Consultation, aspiration and fluid studies
Vancomycin coverage parenterally + cephalosporin vs cefepime, cipro
Median antibiotic treatment in one reported was 14 days
Paronychia
Presentation: Lateral nailfold + extension > runaround
Pathophysiology: Minor trauma (kids)
Pathogens:
Acute
Aerobic and anaerobic bacteria. MRSA/MSSA, strep pyogenes, anaerobes, polymicrobial, pseudomonas, proteus
Chronic: drugs, atypicals
Treatment
With fluctuance: nail considerations
Without fluctuance
Both require warm soaks, elevation, typically antibiotics
Consider culture
Antibiotics
Complicated vs uncomplicated
Antibiotic cream
Coverage of organism discussed above
Bactrim + keflex or dicloxacillin or augmentin vs clindamycin monotherapy
Cellulitis
Epidemiology: Higher risk of hand cellulitis requiring hospital admission
Pathogens:
MRSA and group A strep predominant
MSSA → keflex, dicloxacillin, clindamycin
MRSA → clindamycin, doxycycline, minocycline, bactrim
Special population - IVDU, immunocompromised, clinical toxicity, NSTI
Herpetic whitlow
Clinical diagnosis
Pathogens: HSV-1 or 2
Treatment
No surgical drainage - infection control call for communicable disease
Typically self resolving within three weeks
Immobilization, analgesia, elevation
Antimicrobials - acyclovir, valacyclovir
Consider in recurrent episodes or for immunocompromised
Some studies suggest it reduces duration, recurrence
Little evidence for optical use
Felon
Pathophysiology: Abscesses of the digital pulp
Septa of finger pad > compartmentalization and confine under pressure
Starts with minor trauma → spread along septae → can spread to flexor tendon sheath → flexor teno or osteo, septic arthritis
Think about diabetes
Pathogens: MRSA, MSSA, GAS, anaerobes, polymicrobial
Treat with antibiotics and drainage
Consider observation if concerned about follow up, significant immunosuppression or if prominent cellulitis
Flexor tenosynovitis
Pathophysiology: Infection of space between epitenon layer and parietal layer of flexor tendon sheath
Secondary to trauma, contiguous spread from nearby tissues or seeding from hematogenous infection
Exudative fluid initially → infection setup → purulence of fluid within flexor tendon sheath → ischemic compressive necrosis
Diagnosis: Kanavel signs (91-97% sens in one study)
Ultrasound can help! 94% sensitivity, 74% specificity
Pathogen: Staph most commonly isolated
Treatment includes operative debridement and decompression + antibiotics
Collar button abscess
Pathophysiology: Pain and swelling of webspace → separation of affected digits. Can be dorsal or volar space with typical infectious signs
Often from puncture wound and spread from contiguous area
Pathogen: Staph aureus and GAS most common
Treatment: Hand consult, operative I&D + antibiotics
Animal bites
Dogs/Cats
Epidemiology: 50% infection rate for cats vs dogs rarely cause an infection
Treatment
Consult hand depending on injuries associated
Augmentin, unasyn depending on disposition
Rabies, tetanus, local wound care
Humans
Pathogens: Eikenella corrodens, fusobacterium, peptostreptococcus, Staph aureus
Diagnosis: Consider plain film to assess for retained teeth or foreign body
Treatment:
Presenting more than 8d after injury have 18% chance of requiring amputation
Consultation, antibiotics (augmentin, unasyn vs zosyn vs ceftriaxone + flagyl)
Local wound care
Don’t forget post exposure considerations
r2 qi/kt: dvt WITH drs. comiskey & crawford
Epidemiology
Recurrent DVT occurs in 20-36% of patients diagnosed within 10 years
1-year all cause mortality rate of 4.6 per 100 person-years
Virchow’s triad
Reduced blood flow (venous obstruction, long distance travel, immobility)
Increased coagulability (sepsis, smoking, coagulation disorders, malignancy)
Blood vessel injury (trauma, hypertension, invasive procedure)
Clinical presentation
Swelling in 71%
Cramping, pulling in 53%
Pain worse with ambulation in 10%
Anatomy of the veins of the leg
Common femoral vein
Saphenofemoral junction
Bifurcation of the common femoral vein into the deep femoral and femoral vein
Popliteal vein
Trifurcation of the popliteal vein
Isolated DVT: Implications for 2-Point compression ultrasonography of the lower extremity (n=2400)
Adult patients who received comprehensive lower extremity venous duplex ultrasonographic exam in the ED for eval for DVT
3.9% had SVT, 14.7% had DVT - thrombus was present in more than 1 lower extremity vein in a majority of cases
SVT frequently exists concurrently with DVT in 6-53% of cases and have greater potential to propagate into the DVT system (2.6-15%) or even cause PE (0-33%)
Perform normal DVT US
Image any additional areas of pain/tenderness
Image the proximal 3cm of the greater saphenous vein
If you identify a SVT in the greater saphenous vein <3cm from the confluence of the CFV, save clips and measure the length of the clot
Consider treatment of the SVT as you would for any other DVT identified

If you have a clinical suspicion for DVT, consider calculating a pre-test probability with Well’s Score
If patient has a low pretest probability (Wells score </=1) can rule out DVT with a normal d-dimer
Less than 1% of these patients will have VTE
Not applicable in patients with cancer (2.2% chance of VTE)
If a patient has a high pretest probability (2+), must obtain ultrasound
Venous ultrasonography is first line (but not gold standard); if inconclusive or equivocal will require CT, MRI or contrast venogram
Can EM physicians perform DVT US?
Systematic review that included patients presenting to the ED for suspected DVT and EDP performed ultrasound versus radiology performed ultrasound. [Burnside, 2008]
EDP performed US for DVT with 95% sensitivity and 96% specificity
Prospective study (n=183) in patients with predefined symptoms concerning for DVT
ED performed US has “intermediate diagnostic accuracy” with overall accuracy of 85%; sensitivity 70% specificity 80%
Prospective, cross-sectional study included ED patients with suspected DVT with EDP performing 2 point compression ultrasound versus radiology performed proximal lower extremity duplex US
Accuracy of ED performed US compared to radiology performed US
Systematic review and meta-analysis including patients with suspected DVT
EDP can accurately diagnose DVT with POCUS
Of 16 studies reviewed, 96% sensitivity and 96% spec
Prospective study including patients with moderate or high pretest probability for DVT or a positive d-dimer with EDP performing 3 point compression v radiology
Sensitivity 86%, spec 93%
Multidisciplinary recommendations from the society of radiologist in ultrasound concessions conference - if complete doppler ultrasound is not available in a clinically relevant time frame (EDs, rural areas, off hours) POCUS should be performed if available
A repeat test in 5-7 days is required to evaluate calf veins
ACEP views POC ultrasound for DVT as a core emergency medicine application
Prospective randomized control trial comparing 2-point US with d-dimer to whole leg color doppler ultrasound and noted incidence of VTE during 3 month follow up was equivalent and 2-point US in conjunction with d-dimer is comparable to whole leg US in management and diagnosis of DVT
EDP can decrease time to disposition by 125 minutes if they perform their own US for DVT

Proposed (not yet vetted by quality committee) Qi/KT during lecture
Treatment for DVT

Meta-analysis assessing ED patients diagnosed with low-risk DVT who were discharged with AC versus admission [Khatib, 2020]
Home management was favored with improved mortality, PE, recurrent DVTs and major bleeding events
Total reduction in cost by 56% if discharged home versus admitted
Systematic review comparing patients with diagnosed DVT in the emergency setting who were discharged home with LMWH vs admission with UFH [Cochrane Library, 2018]
Home treatment is no worse than admission with lower rates of VTE recurrence
Retrospective cohort compared patients with primary ICD-10 diagnosis of DVT b location who were discharged home vs admitted [Stein, 2021]
Patients with proximal DVTs and older patients were more often admitted compared to distal DVT or younger patients
Prospective observational study compared patients diagnosed with low-risk VTE who were discharged versus admitted [Beam, 2015]
Xarelto deemed safe for outpatient treatment of low-risk VTE
Hestia Criteria for outpatient pulmonary embolism treatment

Retrospective cohort compared patients diagnosed with isolated DVT who were started on therapeutic anticoagulation versus no AC given [Utter, 2016]
⅔ risk reduction for DVT propagation or PE
Meta-analysis comparing patients diagnosed with VTE on NOACs vs warfarin and placebo [Rollins, 2014]
No significant differences with overall efficacy of anticoagulation; however, warfarin was noted to have significantly worse tolerability
Systematic review and meta analysis compared patients diagnosed with VTE who were on non-VKA oral anticoagulants versus warfarin and aspirin
DOACs were comparable in extended treatment of VTEs, with DOACs having a more favorable side effect profile
EM-PEM COMBINED SIMULATION WITH DR. KETABCHI & PEM COLLEAGUES
Case 1:
Teenage male who presents in wide-complex tachycardia with hypotension after running at football practice. Developed emesis, chest pain and then had a syncopal episode. EMS notes that he is diaphoretic on their arrival. He has received 1/2L of IV NS with noted change in 12-lead EKG to more narrow complex. Has had prior episodes with unremarkable stress tests.
On presentation to the ED patient is tachycardic, hypotensive, and altered. Hr 122, BP 76/44, RR 22, SpO2 90% on RA.
Differential is broad - post-arrest vs tachyarrhythmia. Critical actions on patient arrival to ED:
Prioritizing airway
2 points of access
EKG
Defibrillator pad placement
Bedside TTE demonstrates grossly depressed LV function. Cardiology consultant at bedside concerned about frequent PVCs and ST changes. Decision made to intubate - significant amount of frothy secretions after paralytic pushed, unsuccessful due to obscured view. Successful third attempt.
VBG 7.22/42/57/-2
Mom provides background - similar episode with activity in 2019 with negative EKG and stress test at that time. Suspected neural-related hypotension.
Admitted to CICU and diagnostic cath revealed “slit-like origin of LCA” and he underwent surgery. Post-op TEE showed mildly dilated LV with severely depressed function and started on carvedilol, aldactone, entresto, and farxiga → improved to moderately depressed function.
Epidemiology of heart failure in pediatrics:
12,000-35,000 infants and children/year
11,000-14,000 hospitalizations/year
Etiology:
Cardiomyopathy
1 case per 100,000 children/year
Most are dilated but can be hypertrophic or restrictive
Myocarditis
1-2 cases per 100,000 children/year
Noted in 10-20% of infants with SIDS upon autopsy
Etiology: usually viral with enterovirus, adenovirus, parvovirus B19, SARS-CoV2
A multicenter study demonstrated 45% have chest pain, 45% arrhythmias, 41% viral prodrome, 28% respiratory distress
Evaluation: sinus tachycardia, ST segment abnormalities, T wave inversions, decreased voltages; biomarkers with troponin; CXR
Ischemic
Kawasaki
ALCAPA - anomalous left coronary artery arising from pulmonary artery
Toxins
Anthracyclines - doxorubicin, etc.
Treatment
Unique to disease process
Diuretics and afterload reducing agents
Inotropic support
ECMO or VAD ~60% survival among children with myocarditis requiring ECMO
Managing arrhythmias
Immunomodulatory therapy - IVIG, steroids, etc.
Case 2:
Toddler with complicated cardiac history (“bidirectional Glenn and a lot of other heart surgeries”, cardiac cath 6d ago) with RLE swelling and discoloration. Saturations normally in the 70s. Parents report the patient does not tolerate nasal cannula or simple face masks as it agitates him and that subsequently lowers his oxygen saturations. Patient noted to be grunting on presentation.
HR 155, BP 126/67, RR 31, SpO2 67% on RA
Bidirectional GleNn procedure patients are very sensitive to changes in intrathoracic pressure - be very cautious with any non-invasive or invasive positive pressure application!
Gave patient space. Saturations improved. Had family go back to a private room. Remained HDS and stable on room air. Admitted to cardiology and remained stable on home lasix and losartan. Non-occlusive DVT in RLE and started on lovenox.
For complicated cardiac patients:
Ask family what baseline oxygen saturation is
What is the most recent surgery that the patient has had?
Why are they here?
Single ventricle physiology:
Definition: functionally single ventricle
Other ventricle usually hypoplastic
missing/misplace valves
Etiology: tricuspid atresia, HLHS, DILV, DORV, AV canal defects
Epidemiology: rare but not that rare
HLHS is most common followed by tricuspid atresia
Physiology: variable based on type of lesion
Generally, blood ejected via pulmonary artery which connects to systemic circulation via PDA
Ratio dependent on resistances
Initial management of cyanotic neonate: NRP guidelines
Maintain perfusion and oxygenation
Prostaglandin E1 (alprostadil) to keep the PDA open
Surgical septostomy as indicated
Surgical management:
Stage 1: Norwood
Performed around 1-2 week old
Neo-aorta from RVA with PDA removed, Blalock–Taussig (BT) shunt added: neo-aorta to PA
ASD enlarged: oxygenated blood from RA and RV to neo-aorta
Saturations 75-80%
Murmur from BT shunt - lack of murmur indicates an impending arrest
Impending/current arrest → eCPR
Conventional CPR of limited use due to anatomic abnormalities
Stage 2: Glenn
Performed around 4-6mo old
BT shunt removed
SVC disconnected from heart and attached to pulmonary arteries
IVC filters into RV and goes systemically
Passive flow to lungs...crying increases intrathoracic pressure and blood will not flow to the lungs well causing desaturations
Saturations typically low 80s
Passive return to the lungs - will be decreased by crying or PPV
Children become more cyanotic as they become more mobile
Stage 3: Fontan
18-36mos
Conduit usually added from pulmonary artery
Fenestration from IVC helps with extra blood flow until the lungs adjust
Saturations high 80s-low 90s
Lungs accommodate a higher flow
Still passive return to the lungs




