Diagnostics: Extrapulmonary TB
/Tuberculosis is often thought of as a pulmonary disease, however, Mycobacterium tuberculosis can spread throughout the entire body, causing extrapulmonary tuberculosis (EPTB). EPTB can present with a wide variety of symptoms, often in the absence of any respiratory symptoms. The manifestations of extrapulmonary TB are often indolent and slow to progress, making diagnosis difficult. Delayed diagnoses of EPTB can result in significant morbidity, mortality, and further spread of the disease, making it important for emergency medicine physicians to be aware of what its presentation may look like. This article will review how EPTB is spread, who is at greatest risk, management within the ED, as well as the most common presentations.
Quick Facts
EPTB, like pulmonary TB, is acquired via inhalation of respiratory droplets infected with M. tuberculosis
The bacteria then spread from the lungs systemically via the lymphatic or circulatory systems - this can occur with or without pulmonary infection
Patients with isolated EPTB are generally considered non-infectious, but should still be placed in respiratory precautions
Up to 45% of EPTB cases have a concomitant pulmonary component
13% of patients with EPTB and a negative chest X-ray have positive sputum cultures, indicating active infectious disease
Risk Factors:
Below are the most common risk factors associated with increased odds of EPTB. Patients with these risk factors should have an increased suspicion for extrapulmonary TB, especially when multiple are present.
HIV infection
Odds ratio (OR): 4.93–16.3
Risk increases with lower CD4 counts, especially <200 cells/µL
Female sex
OR: 1.6–1.98
Persistent across geographic regions and independent of other risk factors
Age
Children <15 years: OR 5.50
Primarily lymphatic and CNS disease
Adults >45 years
Higher rates of bone and joint TB
Foreign birth
Most prominent from the Indian subcontinent, Africa, and Southeast Asia
Region of origin may influence disease manifestation
Prior TB infection or known TB exposure
End-stage renal disease
Immunosuppression
Chronic steroid use
TNF-alpha inhibitors
Solid organ transplant
Other immunosuppressive medications
Management in the ED
Place the patient in a negative-pressure room with airborne precautions
Isolation should not be delayed while awaiting imaging
Obtain baseline testing:
Chest X-ray
AFB smear and culture (sputum induction may be required)
NAAT testing
HIV testing
Additional workup should be guided by the individual complaint will be covered below
MOST COMMON PRESENTATIONS
Tuberculous Lymphadenitis
Presentation
Painless, fluctuant, unilateral lymph node enlargement
Most commonly involves cervical lymph nodes
May progress to ulceration, fistula, or abscess formation
Symptoms may be present for up to 12 months prior to diagnosis
Constitutional symptoms (fever, weight loss, night sweats) are often absent
Diagnosis
Fine-needle aspiration or excisional lymph node biopsy is required for definitive diagnosis
Treatment
2 months of RIPE therapy (rifampin, isoniazid, pyrazinamide, and ethambutol) followed by 4 months of rifampin and isoniazid
Temporary enlargement or appearance of new lymph nodes may occur during treatment before improvement
Pleural Tuberculosis
Presentation
Pleuritic chest pain, nonproductive cough, and fever
May also include night sweats, weight loss, dyspnea, and weakness
Can progress to tuberculous empyema
Diagnosis
Chest X-ray typically show a small-to-moderate unilateral pleural effusion
Thoracentesis with pleural fluid analysis:
Elevated LDH (often >500 IU/L)
pH <7.4
Glucose 60–100 mg/dL
Nucleated cell count 1,000–6,000 cells/mm³
Lymphocyte-to-neutrophil ratio >0.75
Adenosine deaminase (ADA) >40 units/L
Treatment
Standard RIPE therapy (2 months) followed by rifampin and isoniazid (4 months)
Pleural drainage may be considered for symptomatic dyspnea
Bone and Joint Tuberculosis
Presentation
Pott disease (spinal TB)
Progressive localized back pain
Commonly affects lower thoracic and upper lumbar spine
Gait changes and postural abnormalities may be present
Fever and weight loss are uncommon
Tuberculous arthritis
Monoarticular swelling, pain, and loss of function
Most commonly affects the hip and knee
Erythema and warmth of joint are usually absent
Osteomyelitis
“Cold abscess” with swelling, mild pain, and minimal erythema
No warmth over the area
Typically affects a single bone
Diagnosis
Definitively diagnosed by microscopy and culture of infected tissue
No pathognomonic imaging findings on MRI or CT
Treatment
Standard RIPE therapy (2 months) followed by rifampin and isoniazid (4 months)
Surgery is often only considered in spinal TB with spinal instability, neurologic compromise, kyphosis, or treatment failure
Important Note
Chronic back pain with new neurologic deficits warrants urgent imaging and specialist consultation
Genitourinary Tuberculosis
Presentation
Renal and urologic TB
Initially asymptomatic with sterile pyuria or microscopic hematuria
Progresses to dysuria, urgency, and frequency
Male genital TB
Testicular swelling, scrotal nodules, or epididymal hardening
Bilateral involvement in up to one-third of cases
Female genital TB
Infertility, abdominal/pelvic pain, menstrual irregularities
Commonly affects fallopian tubes
Diagnosis
CT urography for renal/urologic disease
Biopsy of affected tissue for definitive diagnosis in genital TB
Hysterosalpingogram may aid diagnosis in female genital TB by showing fallopian tube obstruction or uterus deformities
Treatment
Standard RIPE therapy (2 months) followed by rifampin and isoniazid (4 months)
Stenting or nephrostomy tubes for obstructive uropathy
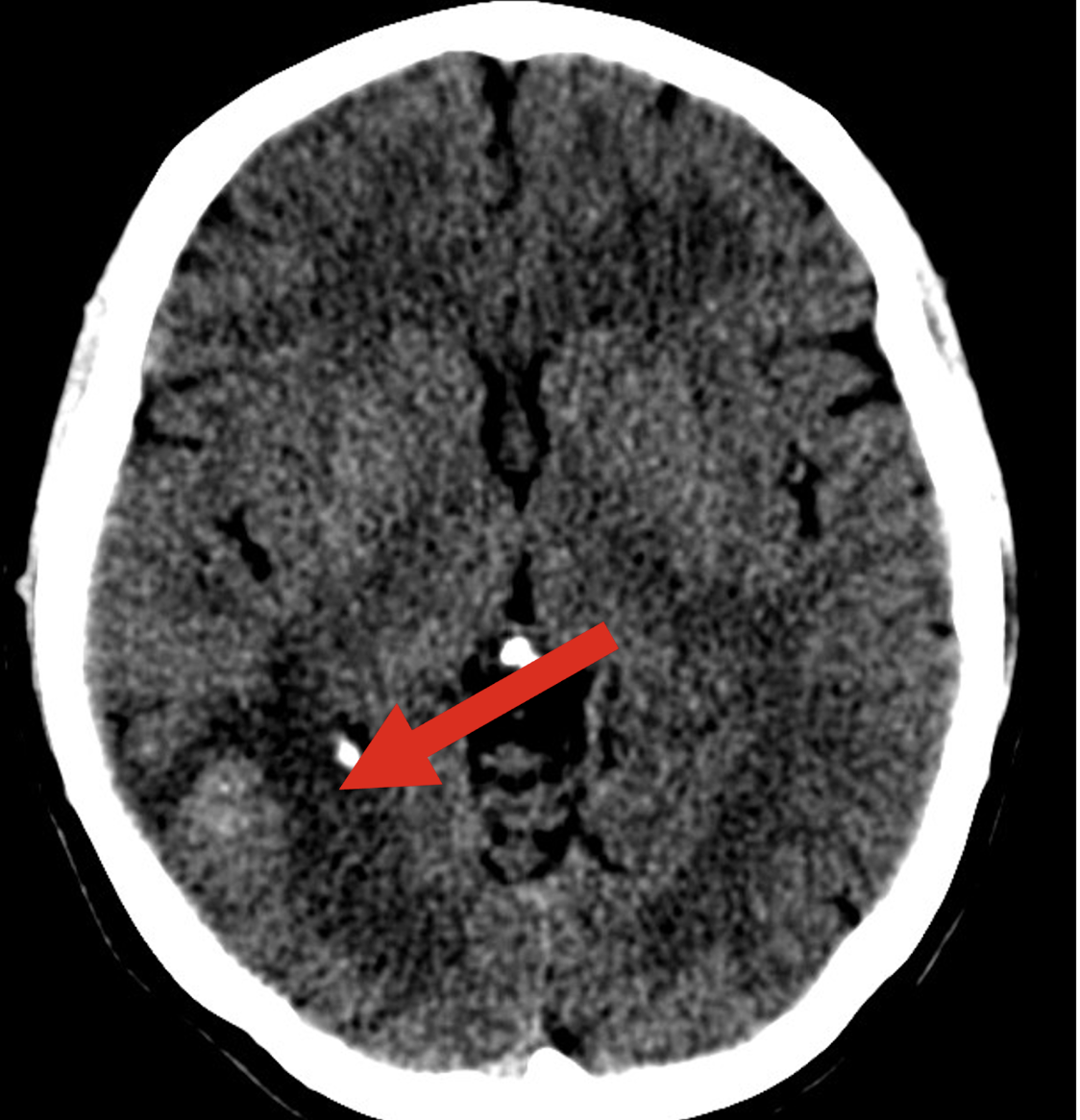
MRI or CT to identify intracranial lesions (Case courtesy of Mohammad Mujalli, <a href="https://radiopaedia.org/?lang=us">Radiopaedia.org</a>. From the case <a href="https://radiopaedia.org/cases/84994?lang=us">rID: 84994</a>) use by CC - SA 3.0
Tuberculous Meningitis
Presentation
Headache, fever, neck stiffness, vomiting
Distinguishing features from bacterial meningitis:
Subacute presentation
Cranial nerve palsies
Altered mental status
Diagnosis
CSF NAAT, AFB smear, or mycobacterial culture
CSF findings:
Lymphocytic pleocytosis
Elevated protein
Low glucose
MRI or CT to identify intracranial lesions (see attached)
Treatment
RIPE therapy for 2 months, followed by 7–10 months of rifampin and isoniazid
Dexamethasone or prednisone for 6–8 weeks
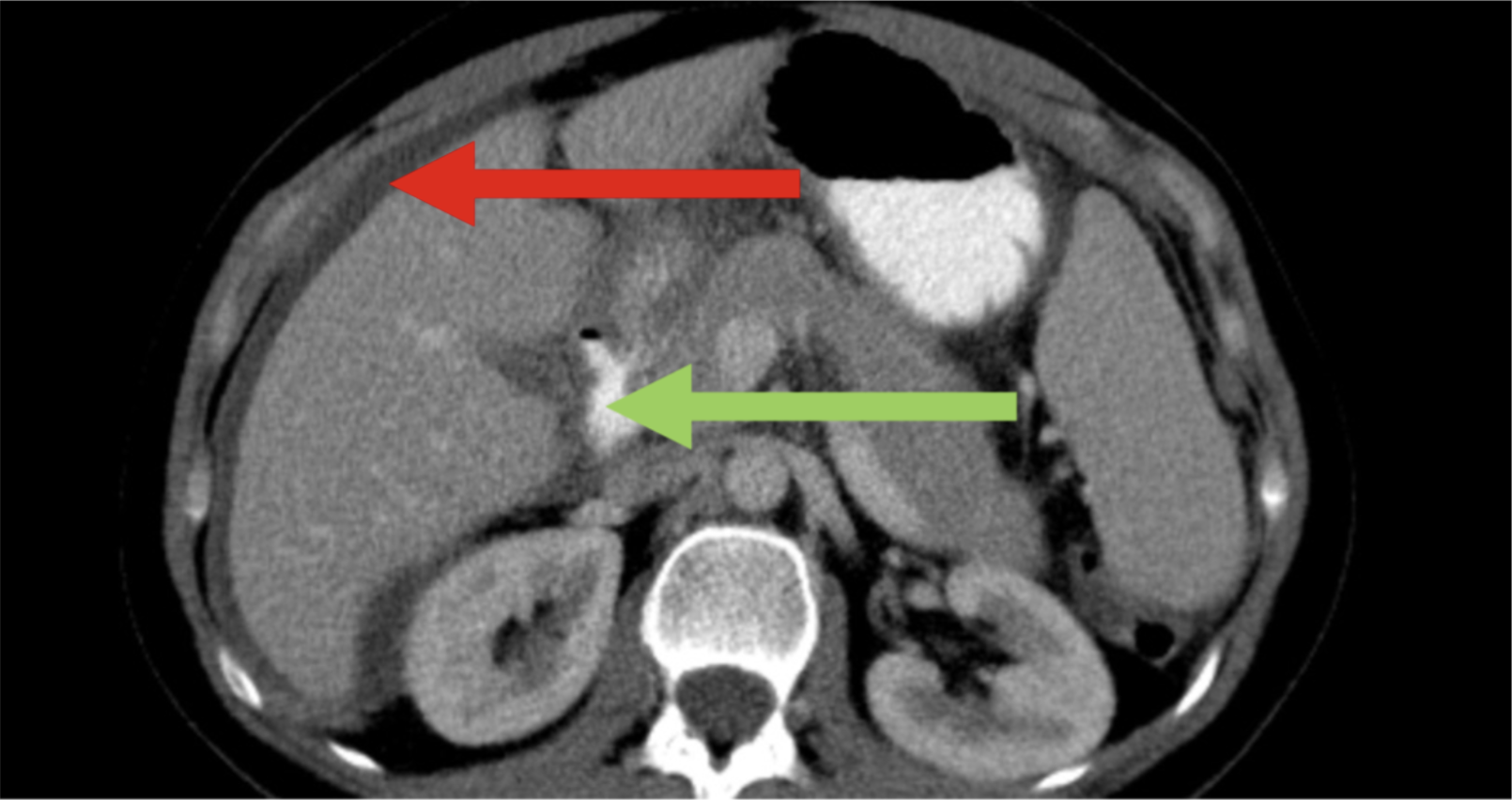
Peritoneal, omental, and mesenteric thickening (Case courtesy of Mohammad Mujalli, <a href="https://radiopaedia.org/?lang=us">Radiopaedia.org</a>. From the case <a href="https://radiopaedia.org/cases/84994?lang=us">rID: 84994</a>) use by CC - SA 3.0
Peritoneal Tuberculosis
Presentation
Ascites, abdominal pain, fever
Advanced disease may present with minimal distension (“dry” phase)
Diagnosis
Definitively diagnosed by peritoneal fluid or tissue biopsy
Ascitic fluid analysis:
Lymphocytic predominance
Serum–ascites albumin gradient <1.1 g/dL
ADA >30 units/L
CT findings:
Ascites (red arrow)
Abdominal lymphadenopathy (green arrow)
Peritoneal, omental, and mesenteric thickening (Case courtesy of Mohammad Mujalli, <a href="https://radiopaedia.org/?lang=us">Radiopaedia.org</a>. From the case <a href="https://radiopaedia.org/cases/84994?lang=us">rID: 84994</a>)
Treatment
Standard RIPE therapy (2 months) followed by rifampin and isoniazid (4 months)
Key Takeaways for the Emergency Department
Extrapulmonary TB often presents without pulmonary symptoms but still needs respiratory negative pressure precautions initially
Maintain suspicion in high-risk populations with subacute or chronic complaints
Isolate early and test broadly
A normal chest X-ray does not rule out TB or infectiousness
References
Shivakumar SVBY, Padmapriyadarsini C, Chavan A, et al. Concomitant pulmonary disease is common among patients with extrapulmonary TB. Int J Tuberc Lung Dis. 2022;26(4):341-347. doi:10.5588/ijtld.21.0501
Le V, Pascopella L, Westenhouse J, Barry P. A Cross-sectional Study of Patients With Extrapulmonary Tuberculosis and Normal Chest Radiographs - What Characteristics Were Associated With Sputum Culture Positivity?. Clin Infect Dis. 2022;75(12):2113-2118. doi:10.1093/cid/ciac338
Peto HM, Pratt RH, Harrington TA, LoBue PA, Armstrong LR. Epidemiology of extrapulmonary tuberculosis in the United States, 1993-2006. Clin Infect Dis. 2009;49(9):1350-1357. doi:10.1086/605559
Wang S. Tuberculous lymphadenitis. In: Post TW, ed. UpToDate. UpToDate; 2026. Accessed February 18, 2026. https://www.uptodate.com/contents/tuberculous-lymphadenitis
Head lymph. Public Domain Media Search Engine. Accessed March 1, 2026. https://garystockbridge617.getarchive.net/amp/media/head-lymph-83d93b
Chopra A, Huggins JT, Hu K. Tuberculous pleural effusion. In: Post TW, ed. UpToDate. UpToDate; 2026. Accessed February 18, 2026. https://www.uptodate.com/contents/tuberculous-pleural-effusion
Visweswaran RK, Pais VM, Dionne J. Urogenital tuberculosis. In: Post TW, ed. UpToDate. UpToDate; 2026. Accessed February 18, 2026. https://www.uptodate.com/contents/urogenital-tuberculosis
Stout, J. Bone and joint tuberculosis. In: Post TW, ed. UpToDate. UpToDate; 2026. Accessed February 18, 2026. https://www.uptodate.com/contents/bone-and-joint-tuberculosis
Ahuja V. Abdominal tuberculosis. In: Post TW, ed. UpToDate. UpToDate; 2026. Accessed February 18, 2026. https://www.uptodate.com/contents/abdominal-tuberculosis
Garg RK. Central nervous system tuberculosis: An overview. In: Post TW, ed. UpToDate. UpToDate; 2026. Accessed February 18, 2026. https://www.uptodate.com/contents/central-nervous-system-tuberculosis-an-overview
Garg RK. Central nervous system tuberculosis: Treatment and prognosis. In: Post TW, ed. UpToDate. UpToDate; 2026. Accessed February 18, 2026. https://www.uptodate.com/contents/central-nervous-system-tuberculosis-treatment-and-prognosis
Garg RK. Tuberculous meningitis: Clinical manifestations and diagnosis. In: Post TW, ed. UpToDate. UpToDate; 2026. Accessed February 18, 2026. https://www.uptodate.com/contents/tuberculous-meningitis-clinical-manifestations-and-diagnosis
Mujalli M, Tuberculosis - multisystem. Case study, Radiopaedia.org (Accessed on 01 Mar 2026) https://doi.org/10.53347/rID-84994
Post by : Tommy Schneider, MD
Dr. Schneider is a PGY-1 in Emergency Medicine at the University of CIncinnati
Editing by : Ryan LaFollette, MD
Dr. LaFollette is an APD in Emergency Medicine at the University of Cincinnati and Co-editor of Tamingthesru.com




