Clinical Concepts in CT Imaging of the Chest
/Case 1

Case courtesy of Dr Craig Hacking, <a href="http://radiopaedia.org/">Radiopaedia.org</a>. From the case <a href="http://radiopaedia.org/cases/35799">rID: 35799</a>
A 45 yo Female presents to the ED with sudden onset of chest pain, described as worse when taking a deep breath. She is significantly short of breath and appears distressed. She recently underwent a total right knee arthroplasty and reports having been bedridden secondary to pain. Physical exam is remarkable for a right lower extremity with surgical incisions that clean, dry, intact; however, her left lower extremity is swollen with significant tenderness along the popliteal fossa and calf.
Vitals: Temp 99.2HR 120RR: 28 BP: 130/80 SpO2 90% on RA.
A CTPA is ordered and shown to the right...
Questions and Discussion
+ Is There a Pulmonary Embolism on this Study?
Yes, this CTPA study demonstrates a large saddle pulmonary embolism with extension into multiple bilateral pulmonary arteries.
+ What are the Diagnostic Criteria for Pulmonary Embolism on a CTPA?
- Arterial occulsion with failure to enhance the entire lumen due to a large filling defect.
- A partial filling defect surrounded by contrast material.
- A peripheral intraluminal filling defect that forms acute angels with the arterial wall.
+ What do "Polo Mints" and Railway Tracks have to do with the Radiographic Diagnosis of Pulmonary Embolism?
The “polo mint” sign refers to a filling defect that is outlined by a rim of contrast when viewing a vessel perpendicular to its long axis.
The "Railway Track" Sign refers to a filling defect outlined by a rim of contrast when viewing a vessel parallel to its long axis.

ATS Diagnostic Evaluation of PE. Leung, et al (2011)
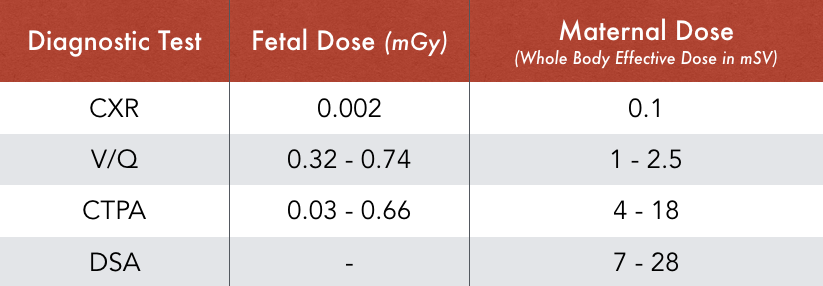
+ The American Thoracic Society Recommends the Diagnostic Approach to Suspected PE in Pregancy seen to the Right. What are the Risks of Radiation to Mother and Fetus Associated with V/Q Scan vs CTPA?
A study performed by Cahill and his colleagues (3) demonstrated that when evaluating a pregnant women with suspicion for PE you were more likely to achieve a diagnostic study with V/Q scan when compared to CTPA nondiagnostic rate of 30% in CTPA vs. 5.6% in V/Q.
Both studies are associated with radiation exposure to mother and developing fetus. A V/Q causes less radiation exposure to the mother relative to CTPA and is largely accounted as another reason V/Q scan is preferred in pregnancy. This is especially important when considering changes in breast tissue during pregnancy as the increased radiation dose is theoretically related to a risk of the development of breast cancer. Although V/Q scan does cause more relative radiation exposure to the fetus it is considered by many experts to be exceedingly small. One Emergency Medicine physician, Dr. Kline (ERcast.org), relates the radiation/cancer risk to money. He states that if 0.1 Gray is analogous to 100 dollars than a V/Q scan would be 50-75 cents and a CTPA would be 25-50 cents. The amount of radiation exposure needed to increase the risk of cancer by 1/10,000 would be 10 dollars. Take home point being that the risk of mortality associated with PE is far greater than the risk associated with radiation exposure to the fetus.
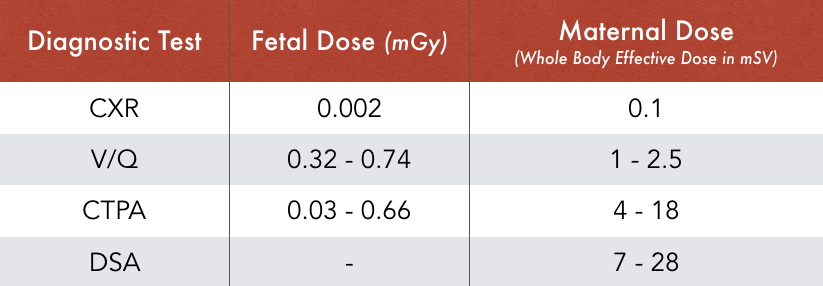
Adapted from Leung, A., et al. (2011)
Case 2
A 60 yo male with a past medical history of uncontrolled hypertension and 100 pk yr smoking history presents to the emergency department with centrally located chest pain described as a ripping and tearing sensation radiating through to his back.
Vitals: Temp: 98.7HR 120BP 160/80RR 25SpO2 96% RA
Physical exam notable for diaphoresis, unequal radial pulses, and a patient who is extreme distress shouting that he is “about to die!”
Chest CT with contrast ordered and can be seen at this link
+ How are Aortic Dissections Classified?
There are 2 main classifications used when discussing aortic dissections: Stanford classification and DeBakey classification.
Stanford Type A
- Involves the Ascending Aorta and/or Aortic Arch
- ~60% of Aortic Dissections
- Surgical Emergency
Stanford Type B
- Involves the Descending Aorta ONLY (Beyond the brachiocephalic vessels)
- Can often be Managed Medically
DeBakey type I: Involves the ascending and descending aorta (Stanford A equivalent)
DeBakey type II: Involves only the ascending aorta (Stanford A equivalent)
DeBakey type III: Involves only the descending aorta (Stanford B equivalent)
Case 3
A 45 year old male, otherwise healthy, is brought to the emergency department following a motor vehicle accident where he was the unrestrained driver and was thrown from the vehicle and subsequently struck by another vehicle.
Vitals: Temp: 99.1HR: 130RR:28BP: 100/70SpO2: 94%RA
Following initial assessment and stabilization patient is sent for CT imaging
+ List some Major Injuries you want to Assess for on Chest CT.
A useful mnemonic for an initial read of a Chest CT is “ABCDEFGHI”
A: Aortic injury (transection)
B: Bronchial injury
C: Cord injury (thoracic spine fractures/malalignment)
D: Diaphragmatic rupture
E: Esophageal injury
F: Flail Chest (Rib fractures)
G: Gas (Air where it shouldn’t be)
H: Heart (cardiac injury)
I: Iatrogenic injury (monitoring for lines/tubes/monitoring adjunct placement)
Additionally, there are more subtle injuries that can be used as indicators of a significant traumatic injury including Scapular fracture, Sternal fracture, Posterior sternoclavicular joint dislocation. Any of these injuries should key you into closer assessment as they would require high impact trauma.
References
- Wittram C, Maher M, Yoo A et al. CT Angiography of Pulmonary Embolism: Diagnostic Criteria and Causes of Misdiagnosis RadioGraphics 2004 24:5, 1219-1238
- http://radiopaedia.org/cases/saddle-pulmonary-emboli-with-right-ventricular-strain-and-pulmonary-infarct
- Cahill A, Stout M, Macones G et al. Diagnosing pulmonary embolism in pregnancy using computred- tomographic angiography or ventilation-perfusion. Obstet Gynecol. 2009. 114:1, 124-129
- ERCAST.org: http://blog.ercast.org/pulmonary-embolism-in-pregnancy/
- http://radiopaedia.org/articles/ct-assessment-of-the-trauma-patient-mnemonic
- http://www.uptodate.com/contents/initial-evaluation-and-management-of-chest-wall-trauma-in-adults#H15009069
- Restrepo C, Gutierrez F, Marmol-Velez J et al. Imaging Patients with Cardiac Trauma. RadioGraphics. 2012. 32:3
Written by: Gerad Colmer, MD
Edited and Posted by: Jeffery Hill, MD MEd




{kind=link}