Grand Rounds Recap - Minor Care Symposium - 9/23
/
This week was a tour of all the little things that make the ED a fun place to work. We're not talking about ECMO or REBOA, we're talking minor care.
Read MoreThis week was a tour of all the little things that make the ED a fun place to work. We're not talking about ECMO or REBOA, we're talking minor care.
Read MoreWhat do I need to assess before I load this patient in the heli?
Sometimes an issue’s theme is evident from the beginning- a well planned coordination of cases and perspectives that delivers a set message. Other times, an issue’s theme develops itself over the course of publishing the issue- a common thread manifests itself to us as editors as the issue comes together. Every so often, as was the case with this issue, AOBP ends up like a B-pod shift itself- a glimpse of the vast and varied pathophysiology that can present to us as Emergency Physcians at any point.
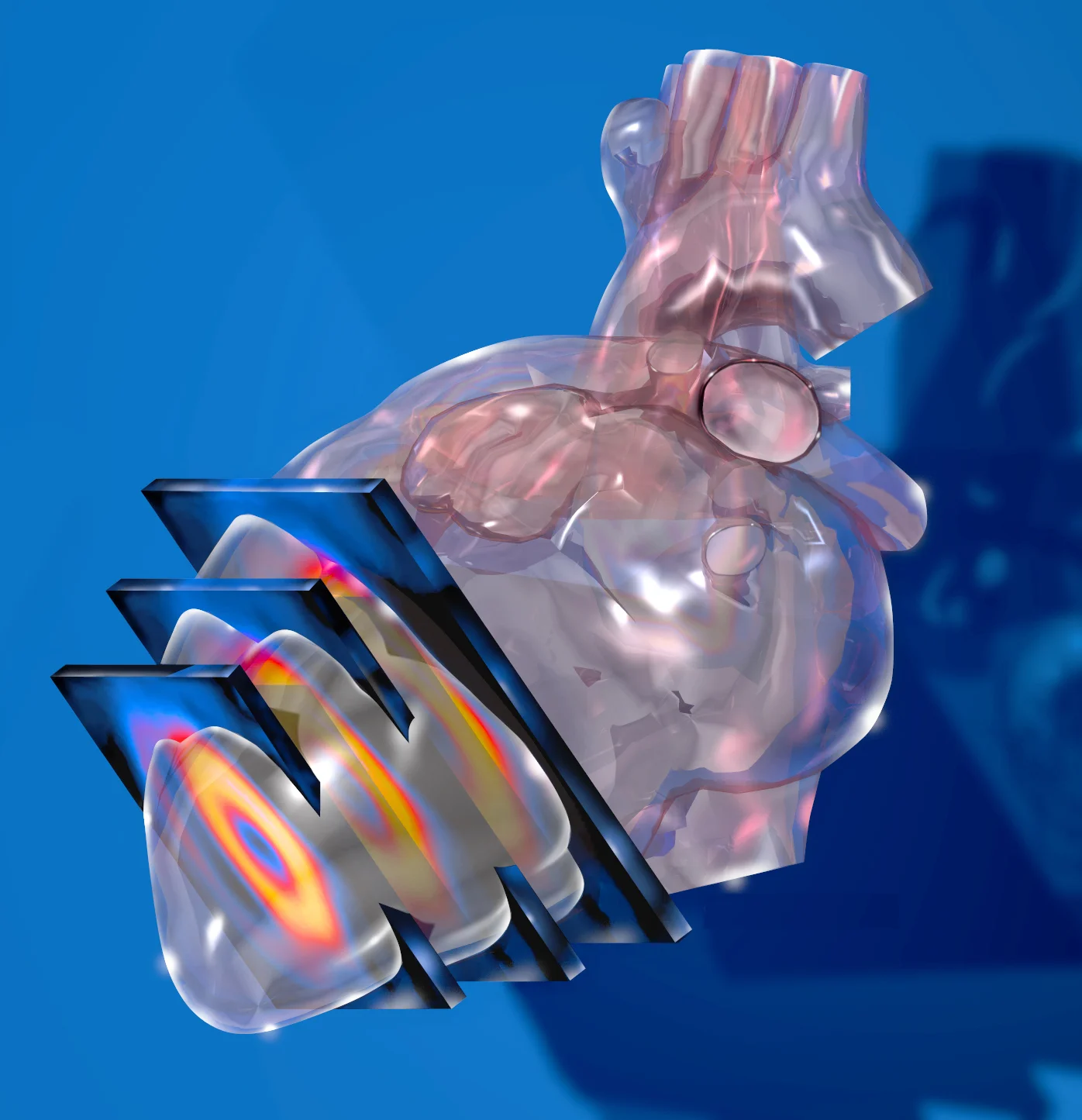
Read MoreThe Sick Patient with Pulmonary Artery Hypertension (PAH)
The patient is a healthy 3 week old male with no past medical history. He was born full term via uncomplicated Cesarean Section who presents with increased fussiness. His mother states the patient has simply not been acting like himself. He was taken home on hospital day 1 without issues, but in the last 24 hours, he has been quite fussy. His mother became concerned when he was unable to take his bottle today. The child has been refusing to eat and has been increasingly difficult to console. He has also had less wet diapers than normal today. Mom has not noticed cyanosis during feeding, recent illnesses or fevers. She also denies the presence of emesis, diarrhea, rashes, congestion, or cough.
Read MoreThe patient is a multiparous female in her 20s, post-operative day 8 from an uncomplicated repeat low transverse cesarean section at 39 weeks gestation after an uncomplicated pregnancy, who presents with SOB. She was discharged home on post-operative day 2 with a healthy female infant. She returns today with complaints of shortness of breath for 3 days and swelling in her bilateral lower extremities for 6 days. Over the same time course she endorses orthopnea, paroxysmal nocturnal dyspnea, weight gain, and chest pain. She describes the chest pain as substernal and intermittent. She also feels as if her chest is making a crackling noise when she exhales. She denies fevers, cough, nausea, vomiting, headache, or abdominal pain. She reports that her incision is healing well. She denies pain or drainage from the incision. She is breast-feeding her daughter, who is doing well at home. She has not yet seen her Obstetrician in follow-up but did receive all appropriate prenatal care.
Read MoreWelcome to Bread and Butter Emergency Medicine; a back to basics, chief-complaint-based podcast series where we get a chance to pick the brains of various faculty members and residents regarding their plan of attack for a particular presenting symptom. Imagine your first shift in the emergency department (or think back on it if you’ve been doing this for a while); a man or woman with the label of “chest pain” or “headache” or “medication refill” is sat down in front of you, staring at you through the glass of your workstation.
Read MoreThe patient is a male in his 20s who was playing soccer and felt a pop in his left knee followed by pain in his left knee. He has not been able to ambulate since the injury. He has an obvious deformity to the lateral aspect of his left knee. His x-ray was read as normal. Given his pain and mechanism, there was concern for fibular head dislocation so a CT of the knee was ordered. This showed an anterior, inferior subluxation of the fibular head.
Read MoreCase 1: Troponin Use in ESRD
ST-elevation in 2 contiguous leads that is:
Men < 40: 2.5 mm ST-elevation in V2 or V3, 1 mm in any other lead
Men > 40: 2.0 mm ST-elevation in V2 or V3, 1 mm in any other lead
Women: >1.5 mm ST-elevation in V2 or V3, 1 mm in any other lead
STEMI's have a 90-minute door-to-balloon time mandate from the Center for Medicare Services (CMS). To be good stewards of our resources we need to be familiar the false positive STEMI patterns. Ultimately, however, some degree of over triage and activation for false positives is expected and (potentially even) desirable.
Read More1) On Technology, Emergency Medicine, and New Frontiers
Today’s tech explosion is leading to health innovations that may make some big differences leading to big changes. Here’s a sneak peak:
In the near future drones may roam the sky to deliver life saving epi pens, defibrillators and instructions of how to use them. Until SkyLab takes over...
Portable ultrasound? Pocket VL? (Hey don't we already have those...)
CHEER Trial: Too young to die? Try ECMO. Australia did and in a trial of 26 people, 14 went on to live and many with excellent neurologic recovery.
TEE: A small number of point of care ED docs are using this successfully to better evaluate causes of shock with good results, low risks (0.03% perf rate), and little training
Thromboelastography (TEG) measures the dynamics of clot development, stabilization/strength, and dissolution. Assuming the body’s ability to achieve hemostasis is a function of these clot properties, TEG provides specific, real-time indicators of a patient’s in vitro hemostatic state. This is in contrast to routine screening coagulation tests such as aPTT and PT/INR which are run with blood plasma alone and therefore do not take into account the cellular components of clotting.
Read MoreSRU (pronounced "shrew") = Shock Resuscitation Unit
Training in, and managing, the SRU is one of the crown jewels of our residency. It is where the sickest of the sick patients are found in our ED. It is a crucible, a test of knowledge and strength, and a true manifestation of the tripartite mission of our department: Leadership, Excellence, and Opportunity.
Training in, and managing, the SRU is one of the crown jewels of our residency. It is where the sickest of the sick patients are found in our ED. It is a crucible, a test of knowledge and strength, and a true manifestation of the tripartite mission of our department: Leadership, Excellence, and Opportunity.