US case of the month - Lung Sonography in CoVID-19
/The Case…
The patient is a 47-year-old male with hypertension and hyperlipidemia who presents to the emergency department (ED) with a chief complaint of cough. He reports a one week history of a dry cough accompanied by subjective fevers, diffuse myalgias, as well as increasing, and now activity-limiting, dyspnea on exertion. His partner had similar symptoms prior to his illness, but recovered without issue. Further he reports dysguesia. The patient reports no lower extremity edema, hemoptysis or pleuritic pain. He has not traveled recently. His vital signs are as follows - temperature of 99.0 F, heart rate of 98 beats per minute, blood pressure 106/77 mmHg, respiratory rate of 20 per minute, with an oxygen saturation of 92% on room air. The physical exam is notable for a mildly uncomfortable appearing male in no acute distress, conversationally dyspneic, with coarse breath sounds that are diminished in the bilateral bases but without focal wheeze. The remainder of his examination is normal.
A thoracic ultrasound is performed at the bedside.
And Now for the Images…
What do you see on ultrasound?
There are five views provided, covering various portions of the left and right lungs. There are diffuse, multifocal B-lines bilaterally, most confluent in the left anterior superior view. The left lateral mid view demonstrates sub pleural consolidation as well as irregular thickening of the pleural line.
Case Discussion
As the CoVID-19 pandemic continues to spread exponentially, and diagnostic resources continue to be a limiting factor, alternative imaging modalities are considered. Although data are limited at this stage, the worldwide Emergency Medicine ultrasound (US) community continues to hold discussions on the role of point-of-care lung sonography in the risk stratification and diagnosis of CoVID-19. This post will discuss the most recent data and expert recommendations on the topics of US machine hygiene, current data on the CT findings of CoVID-19 infection, how they correlate with US and other viral pneumonia syndromes, plus how the sonographic findings (in conjunction with overall clinical picture) may help guide the ultimate treatment and disposition of patients.
The currently well-established diagnostic modalities for the evaluation of CoVID-19 patients in the Emergency Department (ED) other than the overall clinical picture include RT-PCR, plain radiography, and CT scan of the chest. RT-PCR tests may take two or more days to return, thus limiting their utility in the ED. Chest radiography is the standard modality in the ED to evaluate for lung pathology, however it does not perform well in suspected CoVID patients as findings may lag behind the clinical picture. In addition, the use of even portable CXR potentially exposes another staff member to infection. CT is the gold standard for evaluating lung pathology, however, in the setting of a highly infectious agent, its utility is limited by machine availability, extended clean times, and potentially further exposure of staff and even other patients. In this setting, point-of-care ultrasound (POCUS) emerges as a modality which provides an instant result at the bedside, can be performed by the primary provider, and the results can be rapidly incorporated into medical decision making.
Safety first: Current recommendations on ultrasound machine hygiene
The following is based on the ACEP recommendations. Prior to entering the room, all unnecessary probes and objects should be removed from the machine, and a precautionary wipe down of all machine surfaces and all objects remaining on the machine should be performed. Appropriate dry dime should be allowed. An EPA website containing approved wipes and their appropriate dry times is available to the public. There is no current recommendation for the role of sterile probe covers. The machine can then be taken into the room and the examination performed. After the examination is complete, gloved hands should be disinfected and all surfaces and objects on the machine should be wiped down. At this point the machine should be removed from the room, and personal protective equipment (PPE) can be doffed. After donning clean PPE and allowing for appropriate dry time of the initial wipe down, machine surfaces and objects should be wiped down for a third time. After allowing for appropriate dry time once again, the machine can finally be considered decontaminated.
What are the CT findings of CoVID-19?
Zhao et al., in an article in the American Journal of Roentgenology, describe a cohort of 101 patients who had a molecular diagnosis of CoVID-19 pneumonia and had undergone cross-sectional imaging. 86% of these patients were found to have ground-glass opacities, 44% had consolidation, and only 14% showed a pleural effusion. 83% of these patients had bilateral pathology, 55% had multifocal findings, and 32% had diffuse findings. Importantly, 88% of lesions were peripheral, potentially making them amenable to US examination. The authors remark that these findings are not specific to CoVID-19 and are similar to prior studies of other viral pneumonia syndromes.
What are the sonographic findings of CoVID-19 infection?
Studies by Peng et al. and Huang et al., each examining a distinct population of 20 patients in different parts of China, provide the first data on lung ultrasound findings in CoVID-19 pneumonia patients as they correlate with CT findings. They note that their ultrasound findings correlated well with CT findings, are often present prior to any lesions on chest radiography, and are consistent with findings in other viral pneumonia syndromes. The findings, seen in the figures below, include:
Thickened, irregular pleural line, sometimes described as being “ragged” in appearance.
B-lines, the reverberation artifact often described with pulmonary edema - more than three per intercostal space is suggestive of pathology, but confluent B lines should also be concerning.
Sub-pleural consolidations, often multifocal, appearing as hypoechoic “bites” out of the lung parenchyma. This can sometimes be seen in conjunction with hyperechoic air bronchograms, with B-lines emanating distally from the consolidations.
Consistently with the study by Zhao et al. the authors remark that the lesions are often multifocal, multilobar, and are infrequently associated with pleural effusions. The following representative images are derived from the study by Huang et al.
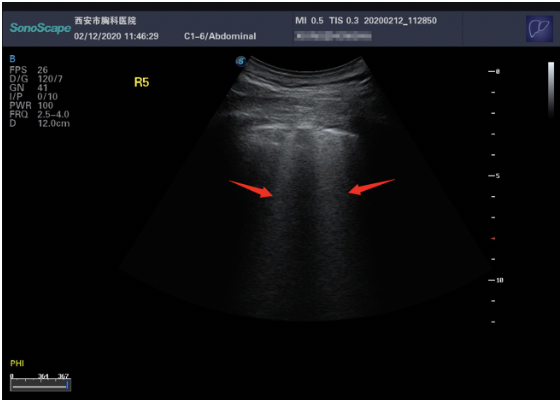
Figure 1. Subpleural b lines, from Huang et a.

Figure 2. Irregular-appearing pleura, from Huang et al.

Figure3. Irregular-appearing pleura with subpleural consolidations and air bronchograms, from Huang et al.
Conclusions
The so far limited data on the role of lung POCUS in CoVID-19 pneumonia patients is retrospective in nature and is based on limited numbers of patients, however it shows an impressive performance of ultrasound as compared to the CT gold standard. POCUS may perform better than chest X-ray, especially early in disease presentation. The ultrasound findings of CoVID-19 infection are similar to those of other viral pneumonia syndromes, and will likely not be diagnostic in the absence of molecular testing. However, in the setting of increased healthcare utilization at this stage in the pandemic, the long return times of molecular tests, the low availability of CT scans and the possibly inferior performance of chest X-ray, there is an emerging role for lung POCUS in the risk stratification of suspected CoVID patients, whether in the Emergency Department, at an Urgent Care, or at an outpatient clinic.
Dr. Mike Stone, founder of the Ultrasound Leadership Academy, proposes an algorithm for the use of POCUS in risk stratification at the point of triage, which is cited below. He advocates for pulse oximetry, rapid influenza testing, CoVID-19 RT-PCR, and ultrasound in patients with a clinical suspicion of CoVID infection or exposure. Certainly patients with a new oxygen requirement must be admitted, however patients with B-lines only may be admitted to a lower level of care, with follow-up POCUS once admitted. Patients with more severe findings, such as sub-pleural consolidations, may be destined for an ICU admission at the time of triage or in the near future. As for patients without an oxygen requirement, the absence of B lines or a presence of A-lines is reassuring for discharge home and self-quarantine. Patients without an oxygen requirement but with B-lines who are clinically well and who may be discharged home will require strict return precautions and close follow-up, whether with primary care or back in the Emergency Department. Certainly all recommendations at this point are based on limited data and will require confirmation with prospective studies at the point of triage, enrolling larger numbers of patients.
Case Resolution
The patient was admitted to the hospital due to concerns for possible progression of his pneumonia. He was started on antimicrobial coverage for potential community-acquired pneumonia. 48 hours after admission his SARS-CoV-2 nucleic amplification assay returned as positive. The remainder of his admission labs were notable for a moderate microcytic anemia, a mildly elevated LDH and a normal ferritin. He intermittently required supplemental oxygen to maintain a normal oxygen saturation, although his symptoms improved rather rapidly. He was able to be discharged with supplemental oxygen on hospital day 3, to complete an oral course of doxycycline for possible superimposed atypical pneumonia. He did well after discharge and weaned from his oxygen without issue.
Take Home Points
Lung sonography may provide a useful tool that minimizes new staff exposure to potential CoVID-19 positive patients.
Findings on ultrasound are generally consistent with other viral pneumonia syndromes, with irregular pleural lines, sub-pleural consolidation, and multifocal B lines
Machine hygiene is essential if utilizing sonography in the general care of patients with respiratory complaints in the age of CoVID-19
Authored by: Michael Gleimer, MD PhD
Dr. Gleimer is a PGY-4 at the University of Cincinnati Emergency Medicine Residency program.
Faculty Edits by: Jessica Baez, MD
Dr. Baez is an Assistant Professor and Assistant Program Director at the University of Cincinnati in the Department of Emergency Medicine.
REferences
ACEP Recommendations for Ultrasound Machine Cleaning. https://www.acep.org/globalassets/images/acep-us-machine-cleaning-covid-19.pdf. Accessed 3/29/2020.
Zhao W, Zhong Z, Xie X, Yu Q, Liu J. 2020. Relation Between Chest CT Findings and Clinical Conditions of Coronavirus Disease (COVID-19) Pneumonia: A Multicenter Study. Am J Roentgenol. Mar 3:1-6.
Peng QY, Wang XT, Zhang LN; Chinese Critical Care Ultrasound Study Group (CCUSG). 2020. Findings of lung ultrasonography of novel corona virus pneumonia during the 2019-2020 epidemic. Intensive Care Med. Mar 12.
Huang, Y, Wang S, Liu Y, Zhang Y, Zheng C, Zheng Y, Zhang C, Min W, Yu M, Hu, M. 2020. A preliminary study on the ultrasonic manifestations of peripulmonary lesions of non-critical novel coronavirus pneumonia (COVID-19). https://papers.ssrn.com/sol3/papers.cfm?abstract_id=3544750. Accessed 3/29/2020.
Mike Stone, MD. CoVID-19 Lung Ultrasound Triage. https://www.butterflynetwork.com/covid-19?utm_source=twitter&utm_medium=social&utm_campaign=covid_landing&utm_content=link_only&utm_term=evergreen#roleofpocus. Accessed 3/29/2020.
Michael Prats. POCUS in COVID-19. Ultrasound G.E.L. Podcast Blog. Published on March 17, 2020. https://www.ultrasoundgel.org/89. Accessed 2/29/2020.
Mike Mallin MD, Jacob Avila MD, Michael Prats MD, Mike Stone MD. Lung Ultrasound in CoVID-19. https://www.coreultrasound.com/usp_covid_1/. Accessed 2/29/2020.



