Grand Rounds Recap - 3/25/15
/Mortality & Morbidity Conference with Dr. Bohanske
Remember that sometimes the thing a patient needs most is a specialist (i.e surgeon), especially trauma patients
![By Photographed by William Rafti of the William Rafti Institute. [CC BY 2.5 (http://creativecommons.org/licenses/by/2.5)], via Wikimedia Commons](https://images.squarespace-cdn.com/content/v1/53c1a2cce4b0e88e61f99b70/1427614248342-UJ3QL7SESVAKCEUJB85O/image-asset.jpeg)
By Photographed by William Rafti of the William Rafti Institute. [CC BY 2.5 (http://creativecommons.org/licenses/by/2.5)], via Wikimedia Commons
- Sharps in hectic situations, such as any resuscitation, are dangerous not just for the patient but also for providers as this is one of the most common situations leading to bloodborne pathogen exposures
- Remove sharps from the field anytime you do not need them and always be responsible for your own sharps to keep your team safe
- Keep in mind that early predicators of hemorrhagic shock are pulse and mental status/anxiety as BP changes are later indicators
- PROPPR was a large RCT of transfusion ratios of pRBC:FFP:platelets of 1:1:1 vs. 2:1:1. While the study did not show an overall difference in mortality, length of stay, or ICU time at 24 hours or 30 days, there was a trend toward patient survival in the 1:1:1 group.
- PROPPR did show that there was increased hemostasis achieved in the 1:1:1 group and less patients died of exsanguination in the first 24 hour with this ratio.
- There was no significant difference in adverse events between the 2 transfusion ratio groups.
- Once hemostasis is achieved one of the best methods to focus on a goal directed transfusion is through a TEG.
- Should our treatment of hemorrhagic shock depend on the cause (i.e. trauma vs. GI bleed vs. menorrhagia)? Probably not.
Anaphylaxis occurs when 1 of 3 criteria occur:
- Acute onset of illness involving skin and/or mucosa with associated respiratory compromise or reduced BP
- Two or more symptoms (i.e. Skin/Mucosa, Respiratory, BP, or GI) after exposure to likely allergen
- Reduced BP after exposure to known allergen
- Epinephrine (0.01 mg/kg 1:1000 IM) is the first line treatment if you believe a patient has anaphylaxis
- Epi can be repeated q5 minutes as needed if symptoms persist or begin a drip for refractory hypotension
- While antihistamines and steroids can help control symptoms neither have shown to be beneficial for treatment of acute anaphylaxis
- While people often get nervous about giving Epi to patients over 50 yo due to concern for cardiac ischemia, no case of this occurring has been documented
Pregnancy induced hypertension occur in up to 20% of pregnancies and 1/4 of those will progress to pre-eclampsia
- Risk factors for pre-eclampsia include previous episodes of pre-eclampsia, first pregnancies, twin gestations, advanced maternal age or family history
- Be sure to evaluate for signs of HELLP by assessing the LFT's, platelets, or hemolysis labs
- Hydralazine should be your first line treatment to acutely lower BP's and do not forget about magnesium sulfate for neuroprotection
Be mindful that the hospital is not always the safest place for patients as adverse events in the hospital are actually quite frequent, such as falls
- Elderly patients are particularly at risk for adverse events due to the many things we consider routine in the ED but are not always necessary for their inpatient course - think twice if patients need monitors attached which can beep frequently keeping patients from sleeping and lines or tubes that can lead to tripping and falling.
Be sure to keep on top of the local EMS protocols as you will often serve as medical command and EMS is an extension of our care
- The SW Ohio Traumatic Arrest Protocol has recently been updated so that field termination of resuscitation is possible in any adult trauma patient who is in bradycardic PEA (HR <40) or asystole.
Tips for Finding a Successful Research Career with Dr. Jesse Pines
Many aspire for academic careers but this can be quite difficult as the research aspect of the mission of academia is rarely taught
- Chart your course by writing a vision statement
- Find a niche which you find interesting and other people will pay you for, but you need to have focus
- Consider various sources of funding including the NIH, Robert Wood Johnson Foundation, SAEM Foundation, Emergency Medicine Foundation
- Find mentors who will help you fulfill your goals and will consider your interests above their own
- Find collaborators as they can enhance your team by providing skills sets that augment your own
- Learn to say no as you may often be asked to do things that can distract you from you mission, so instead trying interesting collaborators in your focus
- Participate in your specialty both inside and outside your institution
- Always ask yourself SW2C (so what who cares) when developing research plans
Common pitfalls researchers will suffer from include not doing an adequate lit review before starting their research, not having a clear question, and not adhering to deadlines
The Affordable Care Act & Emergency Medicine with Dr. Jesse Pines
To understand the effects of the ACA one must first understand the landscape of the American healthcare system and the ED, specifically that we are seeing increasing number of visits and providing increasingly complex and intense care despite a decrease in the overall number of ED's
There are many provision of the ACA including attempts to make healthcare more equitable by regulating certain aspects of the insurance industry (i.e. eliminating lifetime limits of coverage, requiring free primary care coverage, and covering pre-existing conditions), increasing incentives for innovation to increase quality and control costs in healthcare, and expand access to public insurance options through Medicaid expansion
The ACA primarily attempt to create healthcare reform through changes to some aspects of insurance, access, and payment
The ACA will have variable affects on Emergency Medicine including providing more options for patients to going to the ED, increasing focus on value and quality of care, enhancing accountability of providers and ensuring increased coordination of care
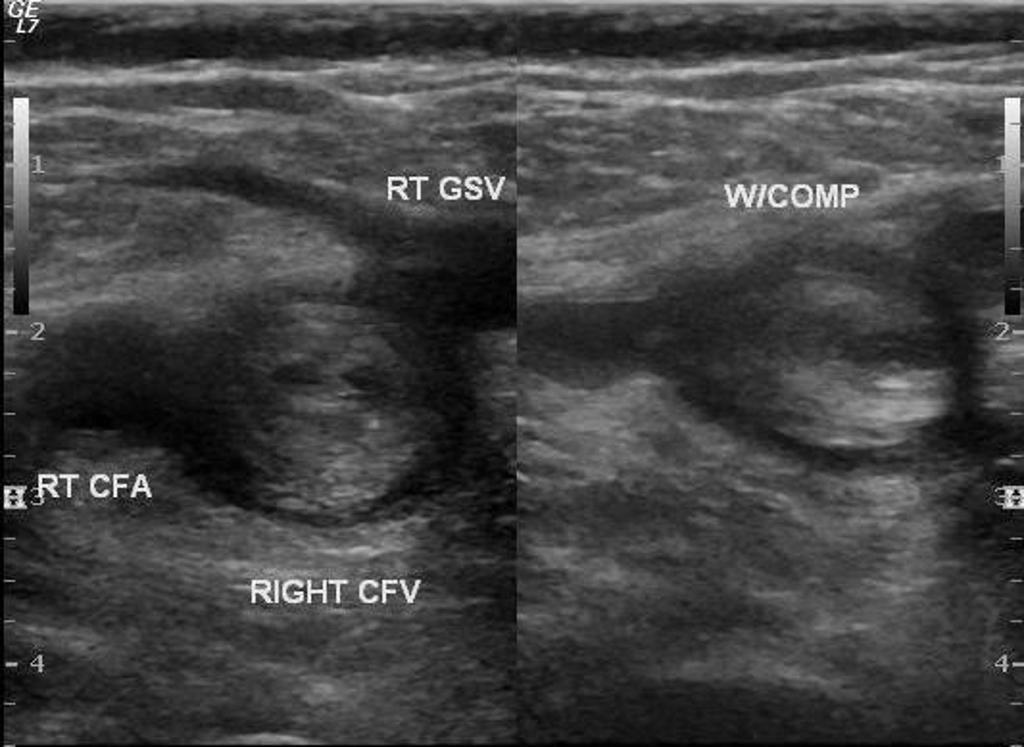
Ultrasound Grand Rounds with Dr. Carleton
DVT is common and has significant morbidity which can be largely preventable if diagnosed early
- US has emerged as the diagnostic modality of choice for DVT detection
- ED physicians are capable of diagnosing proximal LE DVT quickly and accurately with a concordance of 98% to radiology
- Two-point compression US has accuracy similar to whole leg Duplex US for proximal DVT
- Combining Well's score, two-point US, and D-dimer can effectively rule out proximal DVT, thus reducing the need for heparin
- For now, all patients should have a follow-up Duplex study within 5-7 days to detect distal DVT propagation
- To complete a two-point compression US, one must visualize the common femoral vein above, at, and below the saphenous vein takeoff as well as the popliteal vein above, at the level, and below the crease of the knee using the linear high frequency probe
- The folks over at ALiEM published a nice PV Card on this topic recently, navigate over and take a look!
Case courtesy of Dr Ali AbouGazia, Radiopaedia.org. From the case Lower limb deep venous thrombosis (DVT)



