Interpretation of Pulmonary Function Tests in the ED
/Before delving into pulmonary function testing as it relates to the patient in the Emergency Department, let us briefly review the pathophysiology of pulmonary disease.
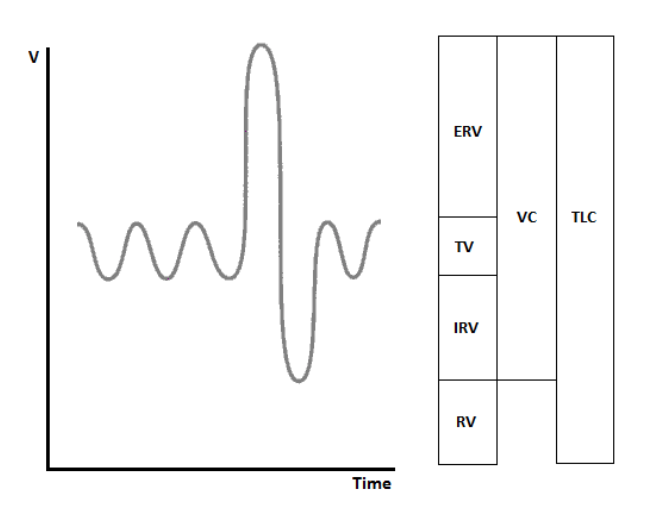
The average total lung capacity 5.8 liters in an adult male and 4.2 liters in an adult female. Of this, only 0.5 liters of air are breathed in and out during resting ventilation, a value known as the tidal volume (TV). The total volume which can be inhaled in on top of the TV is known as the inspiratory reserve volume (IRV). Correspondingly, the volume of air which can be forcefully exhaled below the TV is the expiratory reserve volume (ERV). Together, TV, IRV and ERV make up the vital capacity (VC), the maximum volume of air which can be inhaled or exhaled by an individual. The approximately 1-1.2 liters of air left in the lungs at the end of forceful expiration constitutes the residual volume, which, combined with the vital capacity, makes up the total lung capacity (TLC), the total volume of air in the lungs during maximum inspiration.
Lung pathology in the broadest terms is classified as obstructive or restrictive. In obstructive lung disease — such as asthma, chronic obstructive pulmonary disease (COPD), and chronic bronchitis — the exhalation of air is impeded. In case of COPD, intrathoracic non-cartilagenous airways undergo relative collapse during expiration, due to the inability of damaged surrounding parenchyma to support their patency, thus creating a variable intrathoracic obstruction physiology. Similarly, in the case of chronic bronchitis and asthma, the chronic or acute inflammation of the airway impedes air exit from the lungs. As a result, the rate of air exiting the lungs during expiration rapidly drops, and the expiratory phase is prolonged. TLC in restrictive disease may be preserved or increased due to increased RV resulting from incomplete expiration and air trapping.
On the contrary, in restrictive pulmonary disease there are factors which prevent the full expansion of the lung. These can either be intrinsic pathology of the lung parenchyma, as in interstitial lung disease (ILD) or acute respiratory distress syndrome (ARDS), or extrapulmonary factors, such as obesity, kyphosis, pectus excavatum, or increased intraabdominal pressure. Thus in restrictive disease the rates of air flow in and out of the lung may be near normal, whereas the TLC is decreased.
Spirometry, pioneered in its modern form by the 19th century British surgeon John Hutchinson, is the measure of air flow during respiration. It is a relatively inexpensive test which can be performed in the physician’s office, though it is rarely performed in the Emergency Department. However, when available, this data can be used by the Emergency Physician in evaluation of patients with pulmonary disease. The measurement which helps distinguish restrictive from obstructive disease is the Tiffeneau-Pinelli index. This is the ratio of forced expiratory volume during 1 second (FEV1, the volume of air expelled during the first second of forceful expiration), to the forced vital capacity (FVC, or the total amount of air exhaled). In the healthy lung this index is around 0.8 — in other words, 80% of the vital capacity is expelled in the first second of expiration. Obstructive pulmonary disease is diagnosed when FEV1/FVC is less than 0.7, whereas in restrictive disease it is 0.8 or often higher, due to increased elasticity of the lung in case of parenchymal pathology, such as in ILD.
Once restrictive disease is diagnosed, its severity is measured using the GOLD Severity Scale. This relies on FEV1%, the ratio of patient’s actual FEV1 to predicted “ideal” FEV1, which is based on patient’s gender, height, age and race.
In restrictive disease, TLC can indicate disease severity. TLC cannot be directly measured using office spirometry, as its RV component does not does not directly participate in respiration. It is rather measured using plethysmography, where the patient is placed in a sealed chamber and asked to breathe through a tube connected to a machine outside the chamber. The changes in pressure in the patient’s mouth and in the sealed chamber (reflecting the expansion of the patient’s chest during respiration) can be used to infer the TLC. The normal range of TLC is considered to be 80-120% of predicted.
Another factor commonly reported with pulmonary function testing is the diffusion capacity of the lung for carbon monoxide, or DLCO. This test relies on the extremely high affinity of hemoglobin for carbon monoxide. A patient is asked to breathe in a gas mixture containing a small amount of carbon monoxide, a gas whose ability to cross into the blood is limited by diffusion across the alveoli. The amount of absorbed monoxide is measured. Ideally, this test would reflect the total surface area available for gas diffusion. Its results, however, are also affected by the flow rate of hemoglobin through the lung, and are thus affected by factors such as anemia, polycythemia, V/Q mismatch, and changes in cardiac output. The normal range for DLCO is 80-120% of predicted. In obstructive disease DLCO can be used to distinguish emphysema, where destruction of alveoli results in low surface area for diffusion and decreased DLCO, from chronic bronchitis and asthma, where surface area is preserved. DLCO can also differentiate between parenchymal restrictive lung disease, where alveolar pathology limits diffusion capacity, from extrapulmonary restriction, where DLCO is preserved.
Although extremely useful in evaluating a patients’ pulmonary reserve, formal PFTs are not always readily available in a patient’s record. Over the past century a variety of bedside surrogates for formal PFTs were developed and validated, which include asking the patient to hold their breath and count, recite the alphabet, or blow out a match set at a specific distance from their mouth. Clinical measures, such as the length of a patient’s expiratory phase, can also be used. One of the best validated tests is a simple one: the 6-Minute Walk Test, developed in the 1960s, measures the distance a patient can comfortably walk in 6 minutes. The test can be administered before and after treatment in the Emergency Department, and can involve supplemental oxygen and walking aides as tolerated by the patient. A healthy adult can comfortably walk between 500 and 600 meters in 6 minutes. Although a reduced walk distance is non-specific, and can reflect underlying cardiac and musculoskeletal disease, the test may be a more reliable assessment of the clinical response to treatment in the Emergency Department than oxygen saturation at rest.
References
Godfrey MS, Jankowich MD. The Vital Capacity Is Vital: Epidemiology and Clinical Significance of the Restrictive Spirometry Pattern. 2016. Chest. 149(1):238-51.
Miravitlles M, Roche N, Cardoso J, et al. Chronic obstructive pulmonary disease guidelines in Europe: a look into the future. 2018. Respir Res. 19(1):11.
Han MK, Muellerova H, Curran-Everett D, et al. GOLD 2011 disease severity classification in COPDGene: a prospective cohort study. 2013. The Lancet Respiratory Medicine. 1(1): 43-50.
Johnson JD, Theurer WM. A stepwise approach to the interpretation of pulmonary function tests. 2014. Am Fam Physician. 89(5):359-66.
Stanojevic S, Wade A, Stocks J, et al. Reference Ranges for Spirometry Across All Ages: A New Approach. 2008. Am J Respir Crit Care Med. 177(3): 253–60.
Casanova C, Celli BR, Barria P, et al. The 6-min walk distance in healthy subjects: reference standards from seven countries. 2011. Eur Respir J. 37(1):150-6.
Author - Michael Gleimer, MD PGY-1
Peer Review, Editing, and Posting - Jeffery Hill, MD MEd



