Diagnostics: Musculoskeletal Ultrasound
/Musculoskeletal ultrasound has quickly joined the purview of emergency medicine physicians, and has reshaped our ability to diagnose and treat musculoskeletal conditions. A study of Medicare data from 2008 reported that 30.6% of all musculoskeletal disorders diagnosed via MRI could have been diagnosed with ultrasound[1]. Its advent has expedited care in the department and has the potential to save patients billions of dollars. This article is not meant to be a comprehensive review of the topic, but will highlight a few applications of point of care ultrasound (POCUS) to the diagnosis of musculoskeletal pathology in the emergency department. For a more basic review of ultrasound interpretation, see the Scanning School Studies of TamingtheSRU.
Shoulder Dislocation
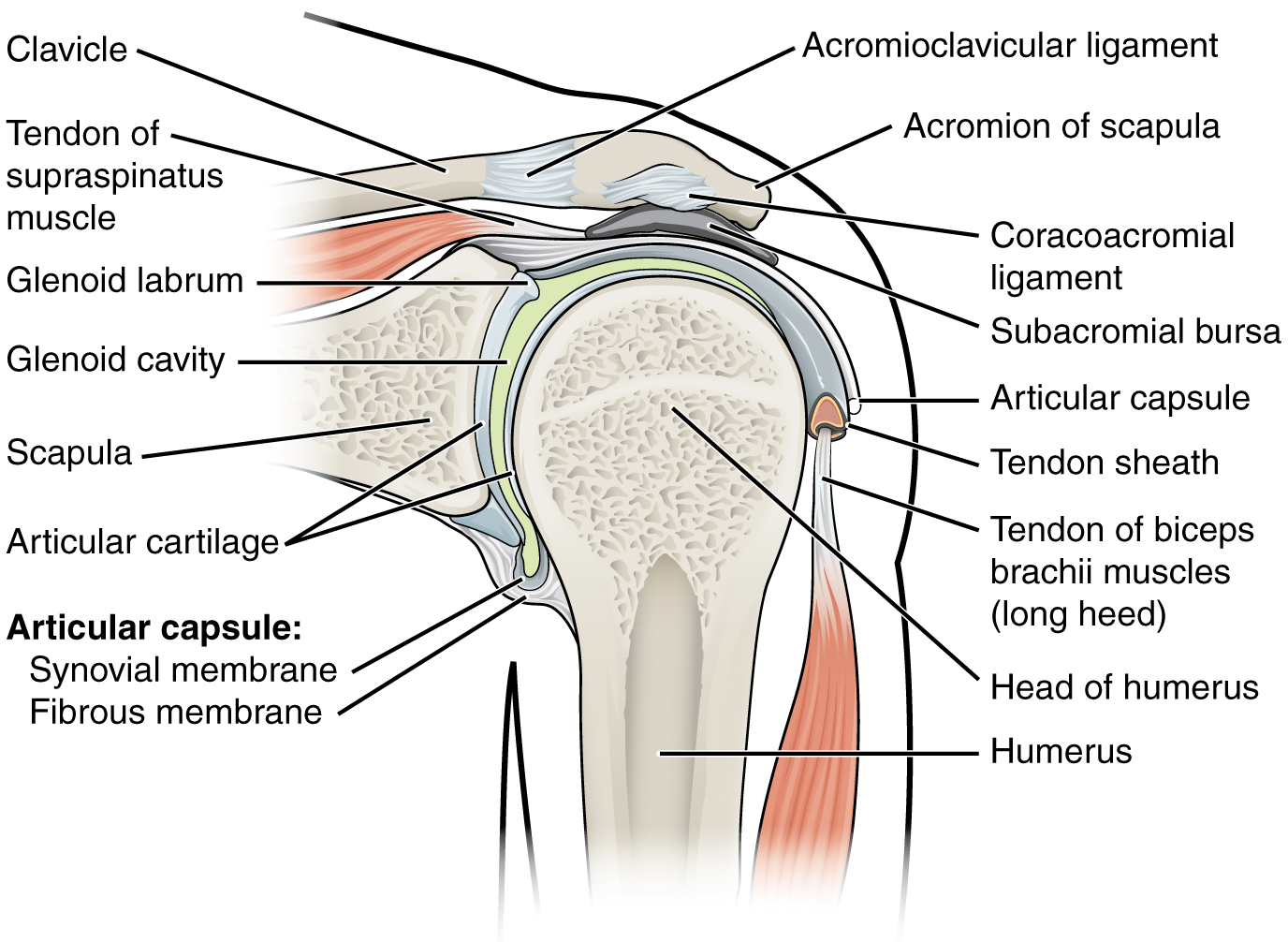
The shoulder joint is composed of a ball and socket joint formed by the head of the humerus and its articulation with the glenoid of the lateral scapula. Surrounding the glenoid is the glenoid labrum, which is a fibrous capsule that increases the surface area for articulation between the humeral head and the glenoid. The proximal humerus also contains insertion points for the rotator cuff muscles, biceps brachii and pectoralis major, teres major and latissimus dorsi, all of which surround the joint. Shoulder dislocations are a common reason for emergency room visits in the United States, and account for approximately 45% of all dislocations [2]. Anterior shoulder dislocations are more common, and occur when a traumatic force is exerted on an externally rotated and abducted shoulder, and secondary contractions of the pectoralis and biceps muscles pull the humeral head anteriorly [3,4]. Posterior dislocations are less common and represent approximately 2-5% of all dislocations, and are usually caused by internal rotation and adduction forces secondary to seizure, electrical shock or trauma.
The shoulder should be imaged with the lower frequency curvilinear probe, positioned in the transverse orientation posterior to the shoulder joint, although if thinner, a linear probe can also be used (as below). First, place the probe, with the indicator facing to the patient’s left, behind the shoulder just under the scapular spine and move laterally until the glenoid is identified. Lateral to the glenoid is the humeral head, which should appear as a circular hyperechoic object with posterior acoustic shadowing. In normal anatomic alignment, the humeral head should articulate with the glenoid such that there is no significant joint space. If the humeral head is in the near field (closer to the footprint of the ultrasound probe), then the humerus is posterior to the glenoid, suggesting a posterior shoulder dislocation. Conversely, if the humeral head is in the far field (further from the footprint of the ultrasound probe) relative to the glenoid, then this suggests an anterior shoulder dislocation. The video below demonstrates reduction of an anteriorly dislocated shoulder. Note that the humerus is initially near the leading edge and the far field (anterior dislocation), and the glenoid is present in the receding edge of the frame separated by hemarthrosis. Additionally, use of ultrasound enables physicians to reliably visualize the joint space to facilitate intra-articular lidocaine for multi-modal analgesia during the reduction attempt.
A recent meta-analysis of 4 studies of ED POCUS use in diagnosing shoulder dislocations revealed 100% specificity across all studies for detecting shoulder dislocation and subsequent reduction [5]. Most studies were 100% sensitive, with the exception of one study that demonstrated sensitivity of 54%, which the authors did note was subject to an array of methodologic flaws. One of these studies also demonstrated POCUS to be a robust tool in diagnosing concomitant shoulder fractures with a sensitivity and specificity of 84.2% and 100% [6]. POCUS can be a useful tool for diagnosis of shoulder dislocation and also for post-reduction confirmation.
Patellar Tendon Rupture
The patellar tendon originates at the inferior pole of the patella and inserts onto the tibial tuberosity. Ruptures of the patellar tendon are uncommon, and the incidence is estimated at < 1% US population per year [7]. The mechanism of injury usually occurs with sudden quadriceps extension and is more prone to occur when the knee is flexed to 60 degrees, often as a consequence of athletic activity [8]. This injury is most commonly seen in patients less than 40 years of age, and may be predisposed by systemic inflammation, corticosteroid use, or previous surgery.
Ultrasound evaluation of the patellar tendon is best achieved with the linear transducer given its superficial position within the extremity. The normal appearance of the patellar tendon will exhibit a linear fibrillar structure with anisotropy, which is a unique property of tendons that appear more hypo/hyper-echoic depending on the angle of insonation as the probe is fanned through the structure. The tendon should appear most hyperechoic with a perpendicular angle of insonation. The tendon is approximately 4-5 mm in anteroposterior thickness and broadens at both insertion points [9]. The tendon should be able to be visualized from the origination site on the patella to the insertion on the tibial tuberosity. Loss of fibrillar structure with defined anechoic and hypoechoic clefts and surrounding anechoic fluid are often preset in partial thickness tears [10]. In addition, significant hyperemia can be present on Doppler imaging. Increased thickness of the tendon at a blind “stump”, or the presence of edge artifact at the site of maximal thickness suggest the presence of a full thickness tendon tear.
The data surrounding ED POCUS use in diagnosing patellar tendon ruptures are limited. A recent blinded retrospective review of 46 ultrasound cases of ED patients suspected to have extensor knee injuries, read by emergency radiologists, proved to have a sensitivity, specificity, positive predictive value and negative predictive value of diagnosing patellar tendon tears of 100% [11].
Necrotizing Fasciitis
Necrotizing fasciitis is a rapidly progressive bacterial infection that spreads along fascial planes and is associated with extreme morbidity and mortality. Check out our prior post on nec fasc. However, not every case of necrotizing fasciitis comes with a LRINIC score > 8 with palpable crepitus, and the diagnosis can often be challenging. Ultrasound can be a useful adjunct to rapidly diagnose this life-threatening condition.
Normal soft tissue should have a homogenous isoechoic echotexture, with hyperechoic planes separating the superficial soft tissue from underlying muscle. With superficial skin infections, ultrasound may be reveal subcutaneous edema, as represented by “cobblestoning”, or anechoic fluid tracking between hyperechoic fat lobules within tissue, highlighting them with a “cobblestone” appearance [12]. This phenomenon is present in peripheral edema, and skin infections including cellulitis and necrotizing fasciitis. However, specific ultrasound findings to suggest necrotizing fasciitis include visualization of gas in tissue planes, diffuse thickened subcutaneous tissue and fluid collection >4mm in depth along the fascial plane [13,14]. Gas within the tissue plane will be visualized as a hyperechoic collection followed by a posterior dirty shadow.
Hyperechoic areas with associated shadowing consistent with a gas forming infection
Currently, the gold standard for diagnosis of necrotizing fasciitis is fascial visualization in the operating room. Quite frankly, the data surrounding diagnosis of necrotizing fasciitis by ultrasound are not robust enough to replace this standard of care. One prospective observational study exists that examined 62 patients suspected to have necrotizing fasciitis, with 17 patients confirmed via fasciotomy/biopsy and found the ultrasound to have a sensitivity of 88.2%, a specificity of 93.3%, a positive predictive value of 83.3%, a negative predictive value of 95.4% [13]. However, this study carried some major flaws, namely that the pathology was limited to extremities, and studies were performed and read only by one ultrasonographer at one institution. Additionally, be aware of mimics like subcutaneous calcifications that can resemble subcutaneous gas with the presence of posterior acoustic shadows [15]. Given these data, ultrasound should not be used as a sole modality to rule in, or rule out this disease, but can be a useful adjunct to supplement clinical decision making in cases of diagnostic ambiguity.
For more cases of ultrasound use in musculoskeletal pathology, here are some TamingtheSRU US posts:
Content by Arthur Broadstock, MD
Dr. Broadstock is a PGY-1 at the University of Cincinnati Emergency Medicine Program with an interest in POCUS
Peer Review and Post by jared Ham, MD and Ryan LaFollette, MD
Dr. Ham is a Chief Resident at the University of Cincinnati and impending Neurocritical Care Fellow. Dr. LaFollette is an Assistant Program Director at the University of Cincinnati Emergency Medicine Program and Co-Editor of TamingtheSRU
References
Parker L, Nazarian LN, Carrino JA, Morrison WB, Grimaldi G, Frangos AJ, Levin DC, Rao VM. (2008). Musculoskeletal imaging: medicare use, costs, and potential for cost substitution. J Am Coll Radiol. 5 (3): 182-8.
Khiami, F.; Gérometta, A.; Loriaut, P. (2015). Management of recent first-time anterior shoulder dislocations. Orthopaedics & Traumatology: Surgery & Research. 101 (1): S51–S57.
Cutts S, Prempeh M, Drew S. Anterior Shoulder Dislocation. (2009). Ann R Coll Surg Engl. 91 (1): 2-7.
Riguzzi, C., Mantuani, D. and Nagdev, A. (2014). How to Use Point-of-Care Ultrasound to Identify Shoulder Dislocation - ACEP Now. [online] ACEP Now. Available at: https://www.acepnow.com/article/use-point-care-ultrasound-identify-shoulder-dislocation/ [Accessed 31 Oct. 2019].
Gottlieb M, Russell F. Diagnostic Accuracy of Ultrasound for Identifying Shoulder Dislocations and Reductions: A Systematic Review of the Literature (2017). West J Emerg Med. 18 (5): 937-942
Akyol C, Gungor F, Akyol AJ, Kesapli M, Guven R, Cengiz U, Toksul H, Eken C. Point-of-care ultrasonography for the management of shoulder dislocation in ED. (2016). Am J Emerg Med. 34 (5): 866-870.
Volpi P. et al. (2016) Patellar Tendinopathy. In: Bisciotti G., Volpi P. (eds) The Lower Limb Tendinopathies. Sports and Traumatology. Springer, Cham
Matava MJ. Patellar Tendon Ruptures. (1996). J Am Acad Orthop Surg. 4 (6): 287-296.
Carr JC, Hanly S, Griffin J, Gibney R. Sonography of the Patellar Tendon and Adjacent Structures in Pediatric and Adult Patients. (2001). American Journal of Roentgenology. 176 (6): 1535-1539.
Berg K, Peck J, Boulger C, Bahner DP. Patellar tendon rupture: an ultrasound case report. (2013). BMJ Case Rep. doi:10.1136/bcr-2012-008189
Petraszko AM, Osborn D, Van Holsbeeck M, Dhillon MK, Kolowich P, and Jacobsen G. Acute patellar tendon ruptures: The diagnostic utility of sonography for tear detection and characterization in the emergent setting (2018). Emerg Radiol. 25 (5):588
O’Rourke K, Kibbee N, Stubbs A. Ultrasound for the Evaluation of Skin and Soft Tissue Infections. (2015). Mo Med. 112 (3): 202-205.
Yen Z, Wang H, Ma H, Chen S, Chen W. Ultrasonographic Screening of Clinically Suspected Necrotizing Fasciitis. (2002). Acad Emer Med. 9 (12):1448-51
Castleberg E, Jenson N, Dinh VA. Diagnosis of Necrotizing Faciitis with Bedside Ultrasound: the STAFF Exam. (2014). West J Emerg Med. 15 (1): 111–113.
Kaiyasah H, Ali MA. Case Report: When all claims that it is necrotizing fasciitis but Point of care ultrasound (POCUS) proves the opposite! (2018). POCUS Journal. 3 (1):13-14.




{kind=link}