Diagnostics: Knee and Ankle X-rays
/Acute Hip Trauma
Hip fractures are a common occurrence and a common reason to seek emergency care. So common, in fact, that they account for nearly 300,000 hospitalizations each year. [1] Typically hip fractures occur from a ground-level fall in elderly and osteoporotic patients. [2]
Indications for X-ray and the Views
The indication is quite simple. Based on the American College of Radiology (ACR) Appropriateness Criteria, a hip x-ray should be obtained for acute hip pain from a fall or minor trauma.[3] Most patients presenting to the emergency department with acute hip pain, whether traumatic or atraumatic, should receive screening plain films to evaluate for an etiology of their pain.

Figure 1 - Case courtesy of Dr Matthew Lukies, https://radiopaedia.org/cases/51246
Plain film may be used to identify the following conditions [4]:

Figure 2 - Case courtesy of Dr Matthew Lukies, https://radiopaedia.org/cases/51246
Pelvis and hip fractures
Avulsion injuries
Hip dislocation
Osteoarthritis and Rheumatoid arthritis
Ankylosing spondylitis
Calcium pyrophosphate deposition disease
Bone tumor
The evaluation for hip x-ray includes two views, the anteroposterior (AP) view of the pelvis and a lateral view with hip flexion (Figures 1,2). [3]
Causes of Hip Pain that Plain X-ray may not Detect
The rule of thumb in acute hip pain is to still order a plain film as the initial imaging modality as most fractures and structural lesions will be seen in this low cost modality. However, there are conditions that cause acute hip pain that will likely not be seen on x-ray, three examples being:
Avascular Necrosis – x-ray is useful to exclude other causes of pain
Septic arthritis – joint aspiration is the most important exam
Osteomyelitis – typically takes two weeks to demonstrate any abnormality
Additional imaging modalities

Figure 3 - hip MRI - Case courtesy of Dr Thuan Tzen, Koh, https://radiopaedia.org/cases/42600
Sensitivity of hip x-ray for an acute fracture is limited. When clinical suspicion for fracture is high and a plain x-ray is negative, additional testing should be pursued. There are several studies that have looked at the incidence of fracture when x-ray was negative. [5,6] It has been estimated that 4-10% of patients with negative hip x-rays will have an occult fracture identified on further imaging. [5]
The additional imaging studies that may be performed to assist clinicians in diagnosing hip fracture when plain radiographs are negative include:
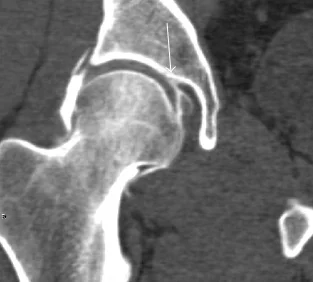
figure 4 - Hip CT - Courtesy of wikimedia.org original available at https://commons.wikimedia.org/wiki/File:Coronal_CT-arthrography_of_ligamentum_teres_tear.jpg
MRI: If a fracture is suspected and the x-ray is negative for acute fracture, the next imaging modality to consider is MRI.iii However, obtaining an MRI in the emergency department can be problematic, depending on the hospital’s availability (Figure 3).
CT: Fortunately for emergency physicians, CT scan of the hip without IV contrast is also appropriate for further evaluation of negative hip x-rays.iii The reason that the ACR lists CT second is due to the balancing of risks and benefits associated with the increased radiation of CT scan versus MRI.[3] However, from an emergency department perspective, CT is typically much easier and quicker to obtain and can increase efficiency and patient throughput. (Figure 4)
Acute Knee Trauma
Acute knee pain accounts for a large number of emergency department visits. In fact, one study found that over 500,000 visits per year were attributed to knee pain.[7] Unlike hip pain, knee pain is more common in the pediatric and adolescent populations.[8] Acute knee pain is most often caused by trauma, followed by infection and crystal-associated inflammation.[8]
Clinical Decision Tools
There are two clinical decision tools for acute knee pain. While using these rules may assist ED physicians to decide when to forgo a plain film, the radiologic evaluation of acute knee pain should always begin with an x-ray.
Ottawa Knee Rule: for patients older than 18 years of age with acute knee pain. If any of the following criteria are met, knee x-ray should be obtained.[9] Several studies have found a 100% sensitivity for acute fracture using this rule (…that’s pretty good).[10,11]
>55 years of age
Palpable tenderness over head of fibula
Isolated patellar tenderness
Cannot flex knee to 90 degrees
Cannot walk in the emergency department (after taking 4 steps)
Pittsburgh Decision tool: for acute knee trauma. Anyone who meets the following criteria should be evaluated with a knee x-ray.[9] The sensitivity of this decision rule has been reported at 92%.[12] The sensitivity is not quite as high as the Ottawa Knee Rule, however, its simplicity may be preferable.
Less than 12 or greater than 50 years old.
Anyone who cannot take 4 weight-bearing steps in the emergency department
Knee Pathology that X-ray May Detect [13]:
Fracture of the knee
Avulsion injuries
Dislocations
Clinically significant knee effusion
Crystal arthropathies
![figure 5 - Lipohemarthrosis on lateral knee - Courtesy of James Heilman, MD [CC BY-SA 3.0 (https://creativecommons.org/licenses/by-sa/3.0)]](https://images.squarespace-cdn.com/content/v1/53c1a2cce4b0e88e61f99b70/1569830126326-AQVHC0IICE2Z64NURVJ5/lipohem.png)
figure 5 - Lipohemarthrosis on lateral knee - Courtesy of James Heilman, MD [CC BY-SA 3.0 (https://creativecommons.org/licenses/by-sa/3.0)]
Additional pathology that X-ray may NOT detect:
Ligament or meniscal tears
Intra-articular pathology (infection, inflammatory conditions, etc)
Occult bone fractures including tibial plateau and tibial spine fracture. A fat fluid level on lateral view may, however, clue you into an occult fracture. [14] (Figure 5)
Chondral injuries
Connective tissue pathology including ligamentous, meniscal, tendon injuries (although avulsion fractures may be apparent on plain film)
Osteomyelitis
Knee XR Views



The two standard views of a knee x-ray are the AP and lateral views
Anteroposterior (AP) view
Lateral view
Tunnel Projection: for suspected fracture of posterior aspect of distal femur.
Sunrise (axial) view: the sunrise (also known as the skyline or patellar view of the knee is most useful in assessing for patellar injury.
Additional Imaging Modalities of Acute Knee Pain:
MRI: most patients who present to the emergency department for acute knee pain have soft or connective tissue injury rather than an acute fracture. Although initial evaluation of any acute knee pain is a plain film, MRI is often indicated on an outpatient basis to identify soft tissue injuries.viii
CT Scan: useful in determining the extent tibial plateau fractures.viii Also useful in trauma patients where position may be difficult for plain films.
Hip and Knee X-ray Quick Hits
For acute hip pain, x-ray is the first imaging modality of choice
X-ray of the hip has limited sensitivity for acute fracture, if initial x-ray is negative for acute fracture, use your clinical suspicion. Depending on your facility, MRI or CT should be obtained
For acute knee pain, x-ray is the first imaging modality of choice. You should obtain AP and lateral views
If suspecting a patellar injury, utilize the sunrise view
For knee soft tissue injuries, MRI is best at detecting any abnormalities and can typically be deferred to the outpatient setting
Post by Kim Gressick, MD MPH
Dr. Gressick is a PGY-1 in Emergency Medicine at the University of Cincinnati
Editing by Shaun Harty, MD and Ryan LaFollette, MD
Dr. Harty is a PGY-4 in Emergency Medicine at the University of Cincinnati. Dr. LaFollette is an Assistant Residency Director at the University of Cincinnati
Other TamingtheSRU posts on this topic include the links below
Clinical Approach to Knee Radiographs by Issac Shaw, MD
How to Read Hip and Pelvis X-rays by Anita Goel, MD
Back to Basics: Pelvic XRays by Sim Mand, MD
References
Tosteson AN, Burge RT, Marshall DA, Lindsay R. Therapies for treatment of osteoporosis in US women: cost-effectiveness and budget impact considerations. Am J Manag Care 2008;14:605-15.
Stevens JA, Anne Rudd R. Declining hip fracture rates in the United States. Age Ageing 2010;39:500-3.
Ross AB, Kenneth KS, Chang EY, et al. ACR Appropriateness Criteria® Acute Hip Pain-Suspected Fracture. Available at https://acsearch.acr.org/docs/3082587/Narrative/. American College of Radiology. Accessed 09/01/2019.
Jude CM, Modarresi S. (2019). Imaging Evaluation of the Painful Hip in Adults. Post TW, ed. UpToDate. Waltham, MA: UpToDate Inc. https://www.uptodate.com
Dominguez S, Liu P, Roberts C, Mandell M, Richman PB. Prevalence of traumatic hip and pelvic fractures in patients with suspected hip fracture and negative initial standard radiographs--a study of emergency department patients. Acad Emerg Med 2005;12:366-9.
Kirby MW, Spritzer C. Radiographic detection of hip and pelvic fractures in the emergency department. AJR Am J Roentgenol 2010;194:1054-60.
Niska R, Bhuiya F, Xu J. National Hospital Ambulatory Medical Care Survey: 2007 emergency department summary. Natl Health Stat Report. 2010(26):1-31.
Tuite MJ, Kransdorf MJ, Beaman FD, et al. ACR Appropriateness Criteria Acute Trauma to the Knee. J Am Coll Radiol 2015; 12:1164.
Cheung TC, Tank Y, Breederveld RS, Tuinebreijer WE, de Lange-de Klerk ES, Derksen RJ. Diagnostic accuracy and reproducibility of the Ottawa Knee Rule vs the Pittsburgh Decision Rule. Am J Emerg Med. 2013;31(4):641-645.
Stiell IG, Greenberg GH, Wells GA, et al. Derivation of a decision rule for the use of radiography in acute knee injuries. Ann Emerg Med. 1995;26(4):405-413.
Stiell IG, Greenberg GH, Wells GA, et al. Prospective validation of a decision rule for the use of radiography in acute knee injuries. Jama. 1996;275(8):611-615.
Seaberg DC, Jackson R. Clinical decision rule for knee radiographs. Am J Emerg Med. 1994;12(5):541-543.
Modarresi S, Jude CM. (2017). Radiologic evaluation of the acutely painful knee in adults. Post TW, ed. UpToDate. Waltham, MA: UpToDate Inc. https://www.uptodate.com




{kind=link}