Grand Rounds Recap 9.28.2016
/Morbidity and Mortality with Dr. Dan Axelson
DKA— The Case: Type I diabetic with pyelonephritis, labs significant for 7.45/30 HCO3 19 AG 19 Glucose 378. Treated with antibiotics, saline, and subcutaneous insulin. Was admitted and re-opened her gap, became acidotic, bumped to step-down on an insulin drip
- To diagnose DKA you do not have to be acidemic, you must have a component of metabolic acidosis. The diagnosis is made with acidosis (AG, low bicarb), ketones, and increased glucose. Our patient had a primary respiratory alkalosis with a concomitant metabolic acidosis
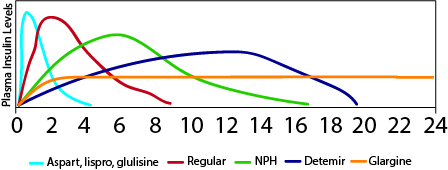
- Should we be using long acting insulin in DKA? Maybe
- In a feasibility study with patients who were in DKA, half were given standard treatment with just fluids and insulin gtt and then the other half got long acting insulin at initiation of the insulin gtt—> no increased hypoglycemia in the intervention group
- Prospective, randomized control study with the experimental group getting basal insulin up front as their gtt was started
- At all time points their sugar was closer to goal range for the interventional group
- They also had less rebound hyperglycemia after the gtt was turned off
- Bolus insulin in DKA? Probably not. At best it doesn't do you any good and at worst it might cause more hypoglycemia
- Prospective randomized study looking at bolus vs non-bolus without any statistical differences but trended towards higher steady state insulin levels
- Prospective observational cohort, half were bolused and half were not and there was a trend towards hypoglycemia in the bolus group
- Asymptomatic hyperglycemia
- Renal threshold: Glucose clamp study that showed people still spill glucose in their urine at 250, usually had to get them below 140 to stop spilling glucose
- Discharge glucose effecting outcomes in d/c patients: retrospective cohort study that looked at any patient with a presenting blood sugar >/= 400 that were then discharged
- 79% got fluids, 69% got insulin
- Mean d/c glucose 334, mean A1c of 10.7
- 40% of patients d/c with glucose >350mg/dL
- In 7 days 13% returned with an ED visit, 7% got hospitalized
- Mean glucose w/ 7 day event: 317mg/dL
- Mean glucose w/o 7 day event: 336mg/DL
TEN— The Case: Young female who presented with pruritic rash, thought to be varicella initially. Returned 2 days later with mucosal involvement and found to have TEN with eventual >95% TBSA involvement thought to be secondary to SLE
- Major Drug Eruptions:
- SJS/TEN
- TEN >30% TBSA
- If they progress to TEN, >95% drug induced and mortality is 35%
- Rarely infections vaccines, autoimmune disease (SLE)
- TEN/SJS Overlap 10-30%
- SJS <10% TBSA
- TEN >30% TBSA
- Staphylococcal scalded skin syndrome (SSSS): confluent, no skip lesions, no mucosal membrane lesions, usually in kids
- Acute Generalized exanthematous pustulosis (AGEP): starts on the face, spreads in hours, mainly pustules
- DRESS: facial edema, spreads out from the face, eosinophilia, hepatitis (10% fulminant—> leading cause of death in DRESS)
- Bullous Disease: discrete bullae, immune mediated and not usually drug related
- SJS/TEN
Suicide in the ED- The Case: Elderly male with a self-inflicted GSW to the head, GCS 3, short hospital course then care is withdrawn
- 43% of people who complete suicide are seen in the ED within one year
- 28% of these people are seen >/= 3 times in the year before completion
- Mean # of visits to the ED in the year proceeding suicide is 3.2
SAD PERSONAS (literature validated scale looking at risk of completion of suicide) *associated with particularly high risk patients
- Sex* (male>female)
- Age (40-65)
- Depression*
- Previous attempt
- Ethanol abuse*
- Rational thinking loss
- Social support lacking
- Organized plan*
- No spouse
- Availability of lethal means
- Sickness
Our social workers also have found the following to be high risk (anecdotally)
- Lower educational status (<high school) *also bears out in the literature
- Times around anniversaries
- If the family concern discordant with patient concerns
- Patients who start lining things up
- Sudden increase in positive mood in setting of depression
They have found the following to be protective:
- Children
- Religion
- Self-presenting
Use the right words
- Did you want to die today?
- How do you feel about your suicide attempt not working?
- Explore the patient’s understanding of their methodology

Outpatient Management of Pulmonary Embolisms— The Case: Patient with PE that is hemodynamically stable, small infarction on CT scan who opts for outpatient management and is started on lovenox/VKA. Returns 24h later with hemoptysis, small amount so admitted and d/c 48h later after he does not cough up any more blood on a heparin gtt.
- Who is appropriate for outpatient PE management?
- HESTIA Criteria— externally validated, if none of the below criteria are met then eligible for outpatient management with Lovenox bridge to VKA (51% of patients screened were elegible). Major bleeding complications .7%, Clinically relevant non-major bleeding 5.1%, Total Recurrence of PEs 2%
- HD Unstable
- Lysed
- Bleeding risk
- O2 requirement for sat >90%
- IV pain meds
- PE on OAC
- Concomitant illness (cancer, CHF, liver)
- Social reason needing admission
- Pregnant
- HIT tx
- PESI Score: Prospective, observational cohort study showed no new VTE, less bleeding with rivaroxaban, 2 deaths unrelated to VTE. NPV 99% for mortality with a score <85.
- Age (age pts)
- Male (+10)
- Cancer (+30)
- Heart Failure (+10)
- Lung disease (+10)
- Pulse >110 (+20)
- SBP <100 (+30)
- RR >30 (+20)
- T <36 (+20)
- AMS (+60)
- O2 sat <90% (+20)
- HESTIA Criteria— externally validated, if none of the below criteria are met then eligible for outpatient management with Lovenox bridge to VKA (51% of patients screened were elegible). Major bleeding complications .7%, Clinically relevant non-major bleeding 5.1%, Total Recurrence of PEs 2%
Hypercalcemia— The Case: Elderly gentleman presents altered, found to have a calcium of 14 and new R lung malignancy
- Levels of Hypercalcemia
- 10-12 mg/gL= mild
- 12-14 mg/dL= moderate
- >14 mg/dL = severe
- Plasma calcium
- Ionized - 50% total (only active fraction)
- Protein bound - 40% total (inactive)
- Complexed Ca - 10% total, bound to phosphate, carbonate, citrate
- Symptoms of hypercalcemia
- General: malaise, weakness, dehydration, polydypsia
- Neuro: confusion, apathy, stupor, irritability, hallucinations, ataxia, hyporeflexia
- Skeletal: fractures, pain, deformity
- GI: nausea, vomiting, abdominal pain, pancreatitis
- Urologic: polyuria, renal insufficiency, kidney stones
- Cardiovascular: bradydysrthymias, QT shortening, ST/T wave coving, widened T wave
- 90% of primary HyperPTH + malignancy
- acutely: malignancy>Hyper PTH
- Treatment:
- Saline Hydration: 200-300ml/h to maintain UOP 100-150cc/h
- Calcitonin: 4 IU/kg will increase renal Ca excretion and decrease osteoclast function. Efficacy limited to 3 doses within 48h
- Bisphosphonates: for malignancy-related hypercalcemia; zoledronic acid 4mg IV over 15 minutes or pamidronate 60mg over 2h
- Lasix: not recommended in absence of renal or heart failure
Pancreatitis— The Case: Middle-aged female with abdominal pain, found to have necrotizing pancreatitis and coded on the floor from her ARDS, ROSC was obtained
- Definition: 1) acute, persistent epigastric pain 2) Lipase >3x upper limit of normal 3) Characteristic imaging findings
- 80% mild, self limiting; edematous pancreatitis
- 20% severe course; parenchymal/peripancreatic tissue necrosis
- infection/sepsis 33%
- bleeding 10%
- abdominal compartment syndrome
- organ failure/ARDs
- Predicting outcomes in pancreatitis
- APACHE
- Ranson’s
- BISAP
- Who to image?
- Ill patients
- >72h out
- Those who’ve had it before
- Does imaging correlate to intervention in acute pancreatitis?
- CTSI is a radiology scoring system that takes into account the amount of pancreatic inflammation, pancreatic necrosis, and extra pancreatic complications which correlates with need for intervention
Pharm Updates with Maddie Foertsch, PharmD
Hereditary Angioedema
- Rare disease (1/10,000-1/100,000)
- Mortality rates are 15-33%
DDx for Angioedema without wheals:
- Hereditary: C1-INH deficiency, Factor XII
- Acquired: Idiopathic, Ace-induced
Patholophysiology: Bradykinin is the mediator, not histamine
Clinical Presentation: acute attacks are usually caused by various known triggers
Patients will present with recurrent attacks of skin swelling, bowel wall swelling, and airway edema. No lung symptoms because bradykinin is metabolized in the lungs
Diagnosis: based on a family history, typical attacks (abdominal attacks sometimes difficult to diagnose), and laboratory confirmation
- C4 level, C1-INH, C1-INH activity
- Reduced C4 and C1-INH low functionality = specificity of 90-100% and NPV of 96%
Treatment options-- Androgens, FFP, TXA were all used prior to development of drugs specific for the disease process. If they have attack at home, they don't necessarily have to come to the ED. They should only seek care if the attack is unusual, the response to self-treatment is inadequate, or if it involves the airway.
Now C1-INH inhibitors are available:
- Ecallantide: kallikrein inhibitor but cannot be given at home because there is a 3-4% risk of anaphylaxis, so their home med is kept in the pharmacy and we give it to them when they get to the ED. Give it early!
- Icatibant: bradykinin B2 recepter antagonist, injection site reaction in 90% of patients
Off-label uses: ACEI induced angioedema. Happens in 0.1-0.7% of people exposed to ACEI and the pathophysiology is thought to be because ACE increases bradykinin levels with a likely defect in some part of the metabolization in those individuals
Icatibant: double blind randomized phase 2 study. Quicker and more commonly complete resolution of acute ACEI angioedema
Exallantide: Not a statistically significant change in discharge times from the ED
Alteplase induced angioedema: 2% of people that get tPA. Plasmin activates C1 and protease that cleaves bradykinin from HMMK, unilateral and usually on the same side as the stroke
Case-Follow Up with Dr. Summers
The Case: Middle aged female with HTN, DM Type I with ESRD s/p failed pancreas and renal transplat, infected dialysis catheter with subsequent endocarditis and CVA. Presents non-verbal, diffuse body pain, and facial swelling, hypertensive otherwise normal VS. Writhing on the bed, facial edema, pupils 6mm and minimally reactive; non-verbal, but non-focal otherwise. TSH 93
Thyroid emergencies: those with thyroid pathology can be thrown from one derangement to the other for a lot of the same reasons. Common causes of derangement include: infection, cardiac, neuro, and drug induced
Thyroid Storm: Labs are not reliable; Tachycardia, AMS, fever, GI symptoms and mimic a lot of other diseases
Treatment: inhibit synthesis, block release, prevent conversion (hydrocortisone), block end organ effects (B-blocker), and supportive care (fever, precipitating events, CHF, or Afib with RBR
Myxedema Coma: Hypothyroidism with bradycardia, hypothermia
Concussions with Dr. Kreitzer
Definition of concussion:

Caused by an impulsive force transmitted to the head
Rapid onset of short-lived impairment of neurological function that resolves spontaneously
May result in neuropathological changes but the acute clinical symptoms largely reflect a functional disturbance rather than a structural injury and no abnormality is seen on standard structural neuroimaging studies.
May or may not result in a loss of consciousness
- Incidence could be as high 3.8 million/yr
- 300K result in LOC
Validated test for concussion include:
SCAT2 (used at the Olympics), Axon Sports, Headminder, imPACT (used in the NFL)
Pathophysiology: Functional and structural
- Axonal injury occurs with the trauma: Axon has increased permeability—>microscopic holes allow issues with both retrograde and anterograde transmission
Neuroimaging: CT usually normal, MRI often normal but autopsies show axonal damage. Because the diagnosis is based on clinical/cognitive symptoms are non-specific and can overlap with a lot of diagnoses, there is a push to find neuroimaging that identifies the damage done during a concussion. Two MRI techniques showing specific aspects of mild TBI:
- SWI (susceptibility weighted imaging) has a 6x time greater ability to see micro hemorrhages in DAI than normal MRI
- Diffusion Tensor Imaging (DTI): sensitive to microstructure changes in the white matter which can reveal microstructure axonal injuries
Clinical Course:
- Most people recover spontaneously
- 15% get post-concussive syndrome
- Chronic Traumatic Encephalopathy (CTE)
- Behavioral: irritability, depression, anxiety
- Cognition: slowed, difficulty concentrating
- Movement: tremors
- Post Concussive Syndrome: highest in patients with history of anxiety, depression, migraines, and prior concussions
Treatment: cognitive and physical rest are the mainstays of treatment--
- Physical rest: animal data, one human study on 95 concussed athletes who retrospectively reported activity. Medium physical and cognitive rest did the best
- Cognitive rest: one study that showed athletes who did better with cognitive rest
- Strict rest: 1 randomized controlled trial 98 patients who had strict rest for 5 days versus usual care (1-2 days rest, then stepwise return to activity)
- Criticisms of rest: What constitutes rest? Does this lead to hyperawareness of symptoms? Somatization? Social Isolation?
- Headache treatment:
- Tylenol/ibuprofen
- Fiorcet*
- Gabapentin
- Sleep problems: melatonin, amitriptyline
NIPPV with Dr. McDonough

CPAP=PEEP used to maintain open alveoli and to effect oxygenation. Improves gas exchange, reduces cardiac after load & direct stress on the heart and reduces work of breathing
Bilevel=PEEP+pressure support. Decreases WOB and increases ventilation.
- Good: Resource utilization, VAP, Airway trauma, Speech & Swallowing
- Bad: Vomiting/aspiration, Secretions, Oral intake/nutrition, Pressure Ulcers
- Really Bad: Delayed endotracheal intubation
COPD: Cochrane review says reduction in mortality and intubation, more rapid lowering of CO2.
- Mental status
- Re-evaluate after 1 hour
Asthma: Cochrane review says no evidence for the use in asthma. May be reasonable to try?
CHF: Cochrane says strong indication for either CPAP or Bilevel. Decreases adverse events but suggestion of possible increased myocardial infarction.
Acute hypoxic respiratory failure: PNA is a predictor of failure of NIPPV
Extubation to NIPPV: COPD mainly as a way to prevent re-intubation from the minute they are exubation. If they are failing extubation, NIPPV actually increases their mortality.
Pre-oxygenation for RSI/DSI: Cochrane says they are better to maintain oxygenation during and after oxygenation
ALI/ARDS: predicted to fail on NIPPV
Critical Care Chalk Talk: End Goals of Resuscitation with Dr. Norton
- When you start resuscitating a patient, have a goal in mind
- Lactate may not be the be all end all of markers of resuscitation
- Resuscitation is all about oxygen delivery
- Delivery of O2= CO x [(1.34 x Hb x SaO2)+0.003 PaO2]
- Attempts to resuscitate should be directed at fixing one of the above parameters




