Diagnostics: GI Bleeding
/
Join Dr. Qin as she reviews the data behind the hot topics in management of GI bleeding, from use of fecal occult testing, imaging and medications to give.
Read MoreJoin Dr. Qin as she reviews the data behind the hot topics in management of GI bleeding, from use of fecal occult testing, imaging and medications to give.
Read MoreNeed a quick reminder of what the MA means as you’re watching your TEG tick by? Join Dr. Della Porta for a quick hit review of Thomboelastography, aka TEG.
Read MoreThe care of trauma patients is constantly evolving. From the time of injury to OR or ICU, there are dozens of management decisions that can improve the care and outcome for your patients. In our most recent journal club we took a look at 3 articles that looked at the management of trauma patients in the ED and ICU. Should we be adding vasopressin to our massive transfusion protocols? Is DL dead for trauma patients? Should we move to use IO’s early in traumatic arrests?
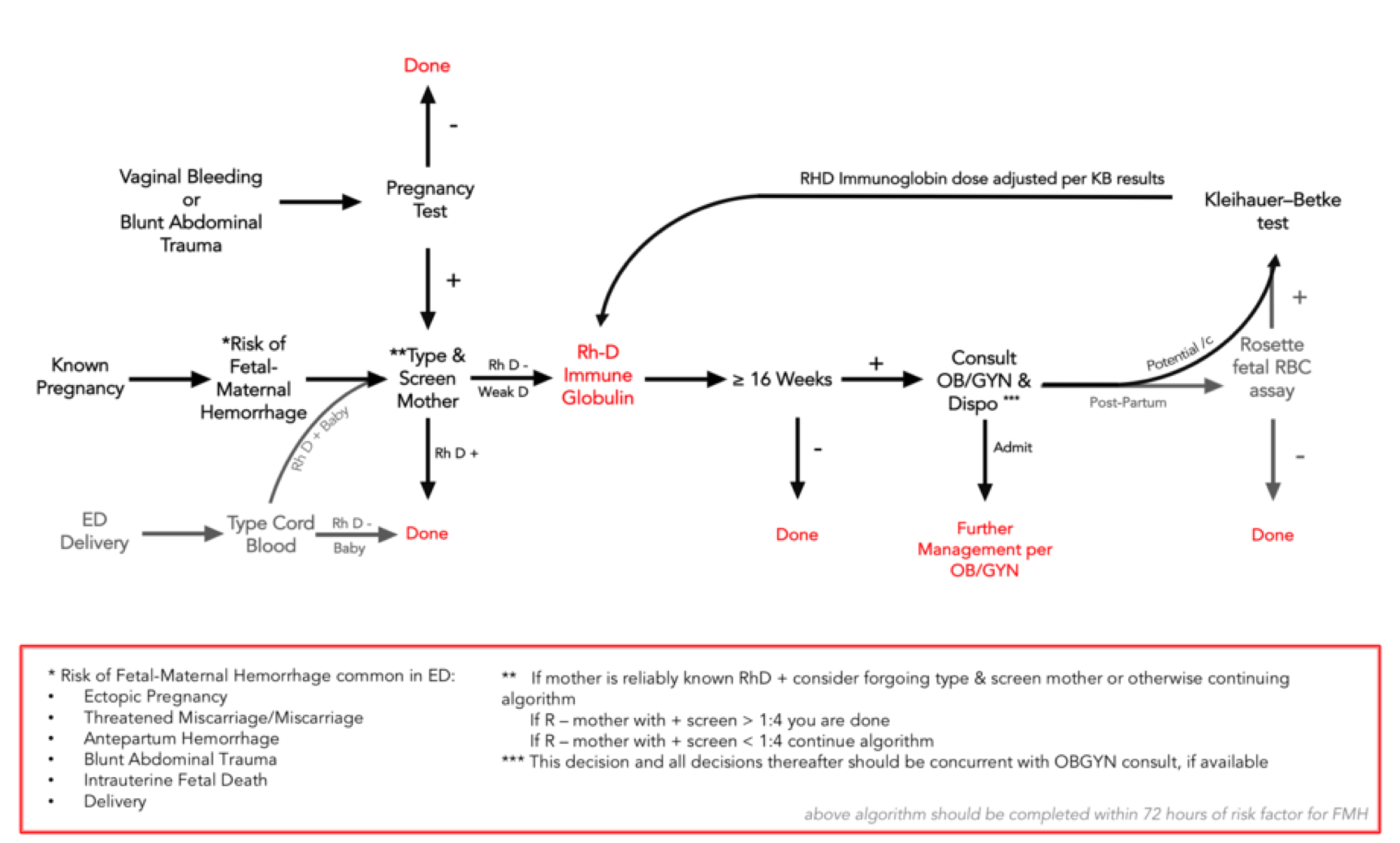
Read MoreHemolytic Disease of the Fetus and Newborn (HDFN) is an alloimmune disease which develops in a fetus when a women’s immune system is sensitized, developing antibodies which cross the placenta and attack fetal RBCs.
While there is a spectrum of the disease, in severe cases the fetus can ultimately develop hydrops fetalis which is often fatal.
As Emergency Physician’s we are classically taught that we can help to prevent HDFN by recognizing sensitizing events in Rh-negative women and subsequently providing RhoGAM. But which patients really need RhoGAM? The evidence seems to be lacking and recommendations are often inconsistent.
Read MoreYou are working overnight as the H2 doc based at Butler County Regional Airport. It’s bitter cold out (for Ohio that is). Its only 11 PM and already the temperature has dropped to 9 degrees fahrenheit on its way to a low of 0. You are in the lounge refamiliarizing yourself with the contents of the critical care cells when the tones go off: “Scene: stab wound – Hamilton Ohio”
You and the nurse grab your equipment, the blood cooler, and head to the helicopter. You put the critical care cells back in their spot in the rear of the helicopter and then buckle in for the short flight to the scene.
Your patient is a 23 year-old female who was in an argument with her boyfriend earlier in the evening. The verbal argument quickly escalated, her boyfrienf pulling a knife and stabbing her multiple times in the right arm and right chest. He fled the scene and she managed to call 911. The first responders found the patient with significant active bleeding from her arm as well as chest. She was initially responsive, but is now only awake to painful stimuli.
You meet the EMS crew in the back of the squad truck and assess the patient from the head of the bed.
Read MoreRadiation effects can be deterministic or stochastic.
To successfully resuscitate the critically ill trauma patient we must have an understanding of and a respect for the LETHAL TRIAD of TRAUMA...
Bleeding causes acidosis, coagulopathy, and hypothermia...
Acidosis and hypothermia causes more coagulopathy which causes more bleeding... and so begins a deadly cycle
Read MoreSRU (pronounced "shrew") = Shock Resuscitation Unit
Training in, and managing, the SRU is one of the crown jewels of our residency. It is where the sickest of the sick patients are found in our ED. It is a crucible, a test of knowledge and strength, and a true manifestation of the tripartite mission of our department: Leadership, Excellence, and Opportunity.
Training in, and managing, the SRU is one of the crown jewels of our residency. It is where the sickest of the sick patients are found in our ED. It is a crucible, a test of knowledge and strength, and a true manifestation of the tripartite mission of our department: Leadership, Excellence, and Opportunity.