The Pancreatitis Case File: From Suspects to Sentencing — An ED Guide to Pancreatitis
/Pancreatitis is the most common gastrointestinal disease requiring acute hospital admission in the United States, generating over 300,000 ED visits per year. A wide variety of "suspects" can trigger the inflammation of the pancreas characteristic of this condition. Join Dr Landry as he investigates types of pancreatitis (acute vs chronic), etiologies, disposition, complications, and treatment for these patients to get to the bottom of the "case" — from mug shots to sentencing.
Opening the case file: acute vs chronic pancreatitis
Acute pancreatitis is a sudden inflammatory process of the pancreas involving adjacent and sometimes distant organ systems. Diagnosis requires ≥ 2 of the Revised Atlanta criteria:

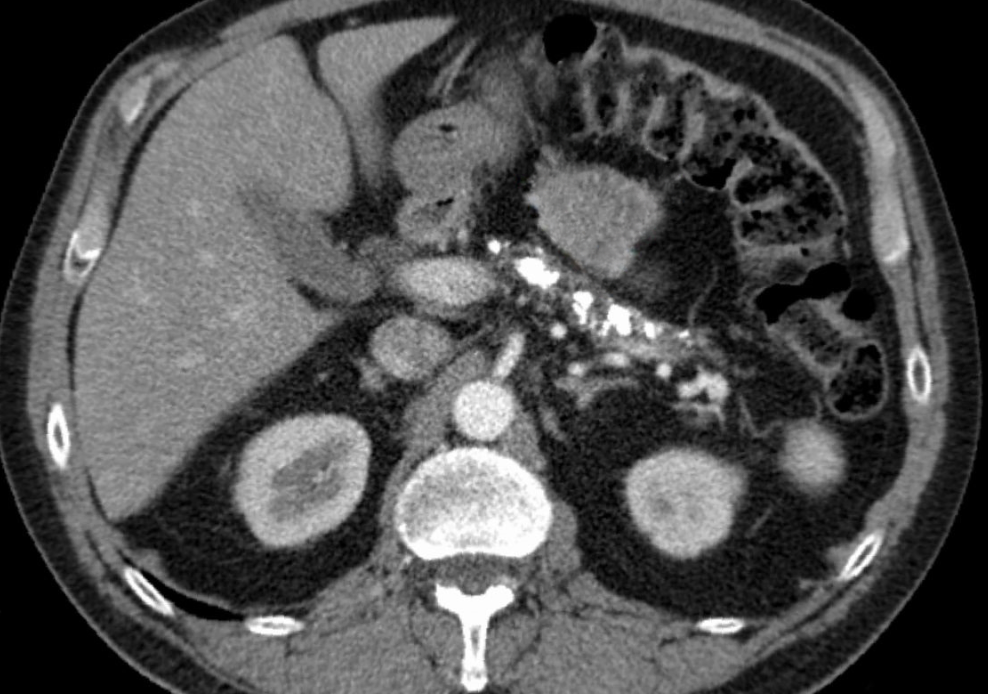
acute pancreatitis - CT findings with enlarged, edematous pancreas and noted stranding / fluid around pancreas; no necrosis noted. image from https://commons.wikimedia.org/wiki/File:Pankreatitis_exsudativ_CT_axial.jpg under Creative CommonsAttribution-Share Alike 3.0 Unported. Accessed June 6, 2026. image edited wth arrow removed from original using canva pro.
Consistent abdominal pain (typically constant epigastric, radiating to the back)
Serum amylase and/or lipase ≥ 3× upper limit of normal
Characteristic findings on cross-sectional imaging (which can include diffuse or focal pancreatic enlargement, peripancreatic fat stranding, or findings of local complications described later in this blog post)
Chronic pancreatitis is a progressive fibroinflammatory disease with irreversible morphologic damage. This is a clinical diagnosis characterized by:
Chronic or intermittent abdominal pain
Steatorrhea and unintentional weight loss
New-onset diabetes from exocrine insufficiency
Often normal lipase but abnormal imaging findings
First-line CT with findings of calcifications, ductal dilation, and parenchymal atrophy
MRI, EUS, and pancreatic function testing can confirm the diagnosis but are typically not performed in the ED
Chronic pancreatitis - CT findings with pancreatic parenchymal calcifications and atrophy
image from https://commons.wikimedia.org/wiki/File:Chronische_Pankreatitis_mit_Verkalkungen_-_CT_axial.jpg under Creative CommonsAttribution-Share Alike 3.0 Unported. Accessed June 6, 2026. image edited wth arrow removed from original using canva pro.
Pearl: Chronic pancreatitis is often — but not always — caused by recurrent acute pancreatitis. Only 30–65% of patients with chronic pancreatitis have documented prior acute episodes. The pathophysiologic theory is that recurrent acute pancreatitis causes repeated pancreatic acinar cell damage, resulting in stellate cell activation and collagen deposition.
The lineup: who is to blame for the inflamed pancreas?
A common mnemonic taught in medical school is I GET PP SMASHED. Here are the suspects, complete with their criminal aliases:
I — Idiopathic
Persona: "The Ghost (Ghostface from Scream)"
Epidemiology: 18% of cases globally.
ED Clinical Pearl: It's only truly idiopathic after a thorough workup. Always rule out occult microlithiasis or biliary sludge via ultrasound before giving up.
G — Gallstones (Biliary)
Persona: "Silent Assassin (John Wick)"
Epidemiology: Most common cause (42% globally).
ED Clinical Pearl: Look for an elevated ALT (greater than 3 times the upper limit of normal), which has a 95% positive predictive value for a biliary cause. Get that Right Upper Quadrant ultrasound in the ED.
E — EtOH / Alcohol
Persona: "Repeat Offender (Frank Gallagher in Shameless)"
Epidemiology: Second most common cause (21% globally).
ED Clinical Pearl: Usually requires years of heavy alcohol intake. Chronic baseline changes can mask acute flares on imaging, so trust your clinical exam and trends.
T — Trauma
Persona: "Blunt Force (Incredible Hulk)"
ED Clinical Pearl: Classic pediatric or handlebar injury scenario. The pancreas gets compressed right against the vertebral column. Lipase can be normal initially post-trauma, so serial exams matter.
P — Posterior Duodenal Ulcer Rupture
Persona: "Backdoor Breacher (Ocean's Eleven Crew)"
ED Clinical Pearl: This is a localized chemical pancreatitis caused by gastric acid leaking directly onto the pancreatic head from an adjacent perforation.
P — Pancreatic Divisum
Persona: "The Congenital Con Artist (Marvel's Loki)"
ED Clinical Pearl: The most common congenital pancreatic anomaly. Failure of the dorsal and ventral ducts to fuse forces the majority of secretions through the tiny minor papilla, leading to relative obstruction and inflammation.
S — Steroids
Persona: "The Juice (Lance Armstrong)"
ED Clinical Pearl: A rarer medication-induced cause. Keep it on your differential for patients on chronic high-dose immunosuppressive regimens or acute pulses.
M — Mumps & Other Viruses / Malignancy
Persona: "The Infiltrator (The Thing)"
ED Clinical Pearl: While mumps is classic for board exams, in the ED, think malignancy for older patients presenting with their first episode of 'idiopathic' pancreatitis without an obvious cause.
A — Autoimmune Disease
Persona: "The Double Agent (Severus Snape)"
ED Clinical Pearl: IgG4-related disease is the classic culprit here. It often mimics pancreatic cancer on imaging (forming mass-like lesions) but responds beautifully to steroids.
S — Scorpion Stings
Persona: "Exotic Hitman (Spider-Man's Scorpion)"
ED Clinical Pearl: Specifically from the Tityus trinitatis scorpion in Trinidad. It hyper-stimulates pancreatic exocrine secretion. A pure board exam favorite!
H — Hypertriglyceridemia
Persona: "The Rich, Greasy Villain (Jabba the Hutt)"
Epidemiology: 2–5% of cases; highest risk of severe disease.
ED Clinical Pearl: Triglyceride levels must typically be greater than 1,000 mg/dL to trigger this. Beware: ultra-high lipid levels can cause a falsely normal serum lipase reading due to assay interference!
E — Post-ERCP
Persona: "Iatrogenic Inside Job (The Departed)"
Epidemiology: 5–10% risk with ERCP; mildest etiology.
ED Clinical Pearl: Mechanically and hydrostatically induced. Fortunately, it is usually the mildest etiology, but it requires post-procedural monitoring if a patient presents to the ED with severe back pain.
D — Drugs
Persona: "Shady Dealer (Walter White from Breaking Bad)"
ED Clinical Pearl: Think of the classic offenders: Azathioprine, Valproic Acid, Diuretics (Furosemide/Thiazides), and HIV medications (Didanosine). Always run a thorough med-reconciliation.
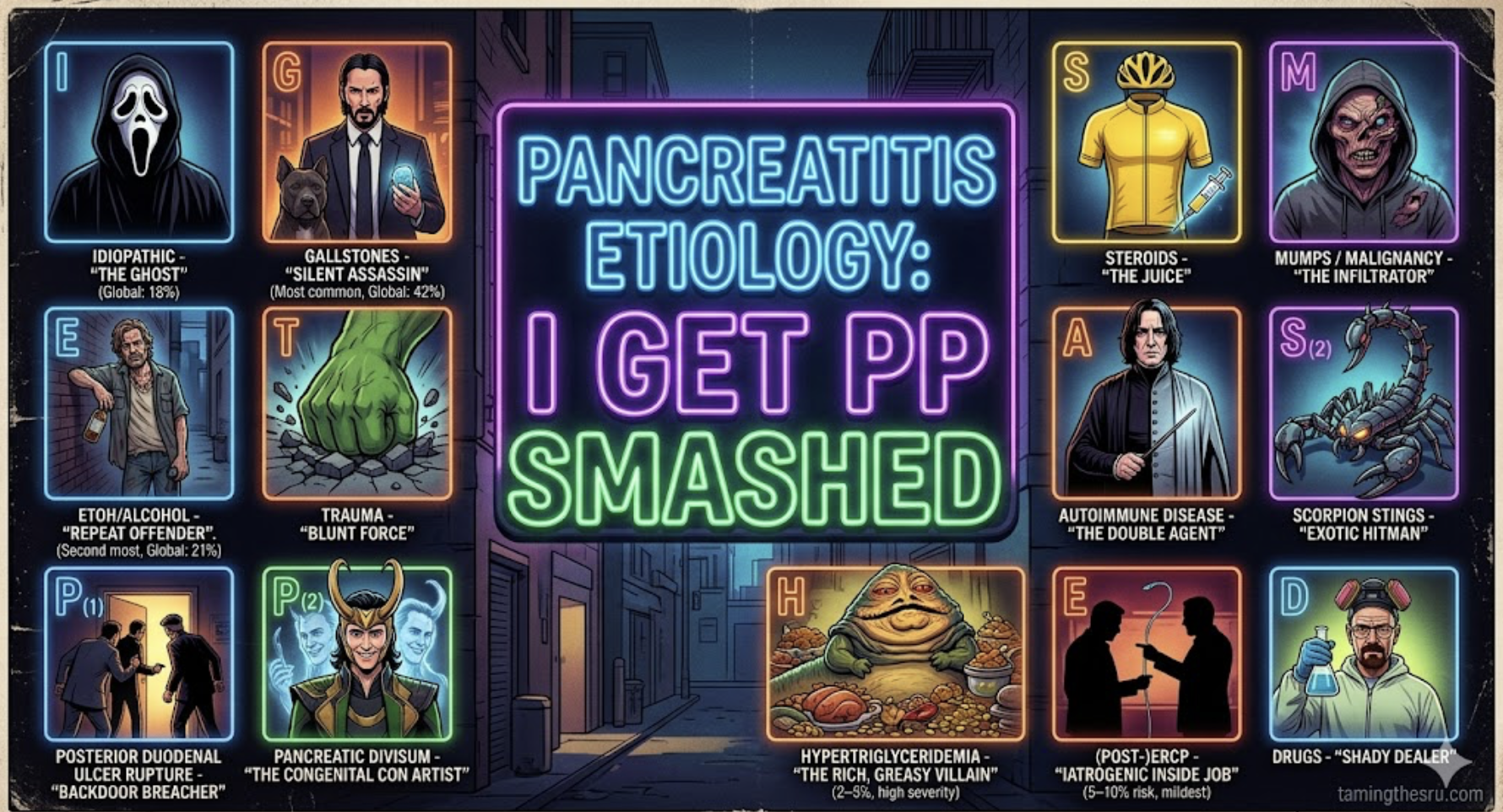
original image created by google gemini AI tools
Remember: Hypercalcemia can also cause pancreatitis and is often included in the “H” of the mnemonic. AND If you remember nothing else for a busy shift, remember that Gallstones and Alcohol account for nearly two-thirds of all cases. If it's neither of those, look for the "Greasy Villain" (Triglycerides > 1,000 mg/dL) or an "Infiltrator" (Malignancy) in older adults.
Pearl: Hypertriglyceridemia-induced pancreatitis carries the highest risk for non-mild disease and the greatest mortality of all etiologies.
Sentencing: severity classification and disposition
We've rounded up the suspects — now, how serious is the crime? Before we investigate the full scene or begin treatment, we need to classify the severity to determine where these patients are headed.
Pancreatitis has a bimodal mortality pattern: early deaths are driven by SIRS and early organ failure from the systemic inflammatory cascade, while later deaths are driven by infected necrosis and sepsis-related organ failure. The severity classifications for mild, moderate, and severe pancreatitis below are driven by the “Revised Atlanta Criteria”. Chronic pancreatitis, also below, is not included in this classification system.
1) Mild Acute Pancreatitis — self-limiting, no organ failure or local complications
This accounts for ~80% of cases. These patients should either be discharged or admitted to a floor unit.
A few scoring tools help identify patients with a non-severe course:
Harmless Acute Pancreatitis Score (HAPS) can identify patients within 30 minutes of arrival using three parameters: no peritonitis (lack of rebound or guarding), normal hematocrit, and normal serum creatinine. A meta-analysis of 20 studies found HAPS had a PPV of 97% for identifying non-severe AP and 98% for predicting a non-fatal course.
BISAP score (BUN >25, altered mental status, SIRS, age >60, pleural effusion) is complementary — a score of 0 is associated with 1% mortality. However, this score predicts severity rather than safe discharge.
Who can go home? The best available prospective data comes from Beth Israel, which used a 5-year tertiary center protocol and found decreased mean ED length of stay (12.3 vs 116 hours) and mean charges ($6,768 vs $19,886) with no difference in 30-day readmission rates for patients discharged from the ED via an observation pathway.
The strongest predictors of successful ED discharge were:
Age 50
Charlson Comorbidity Index < 2 (weighted score of 19 comorbid conditions based on strength of association with 1-year mortality)
Non-biliary etiology
Idiopathic acute pancreatitis (OR 7.8 for successful discharge)
2) Moderately severe acute pancreatitis — transient organ failure 48 hours and/or local complications (carries ~2% mortality)
These patients should generally be admitted to a step-down unit. Important caveat: the distinction between "transient" and "persistent" organ failure inherently requires up to 48 hours of observation, so this classification cannot be definitively made in the ED. What we can do is identify organ failure at presentation (can use the Revised Atlanta Classification’s grading tool called the modified Marshall score which evaluates dysfunction in three organ systems – respiratory, renal, and cardiovascular – each scored from 0 to 4, with a score ≥ 2 in any system defining organ failure - pictured below) and initiate an appropriate disposition. If a patient has organ failure in the ED, they should be managed as potentially severe until the clinical trajectory clarifies over the next 48 hours. Patients whose organ failure resolves within 48 hours are reclassified as moderately severe; those whose organ failure persists beyond 48 hours are classified as severe.
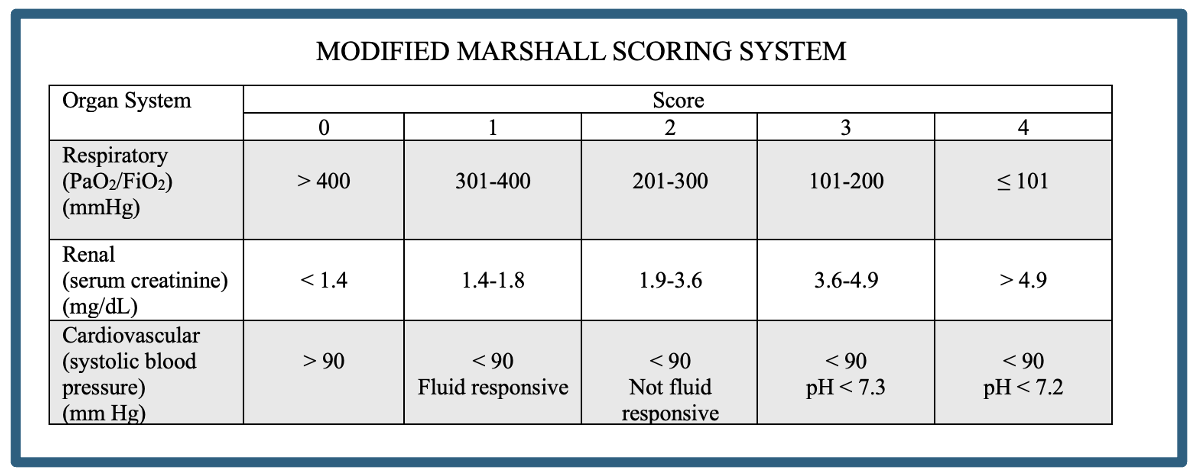
original table created by author.
This is the modified Marshall scoring system which is a grading tool specifically incorporated into the Revised Atlanta classification for acute pancreatitis. A score of ≥ 2 in any system defining organ failure. These patients would be classified as moderately severe or severe depending on the duration of organ failure.
3) Severe acute pancreatitis — persistent organ failure >48 hours with high mortality at 25–46%
These patients typically require the ICU. Consider ICU admission if the patient has:
Pulse < 40 bpm or > 150 bpm
SBP < 80 mmHg or MAP < 60 mmHg or DBP > 120 mmHg
RR >35/min
PaO₂ < 50 mmHg
pH < 7.1 or > 7.7
Na < 110 or > 170; K < 2.0 or > 7.0
Glucose >800 mg/dL; calcium >15 mg/dL
Anuria or coma
Pearl: Severity staging in pediatrics mirrors the adult Revised Atlanta Classification with moderately severe or severe acute pancreatitis occurring in approximately 13-30% of pediatric cases.
4) Chronic Pancreatitis Disposition
Patients with chronic pancreatitis are less likely to be admitted (~63% of ED visits result in admission). Admission is determined by acute complications or symptom severity. Consider admission if:
Acute-on-chronic pancreatitis (manage per acute pancreatitis guidelines above)
Intractable pain beyond outpatient management
Complications requiring inpatient intervention (pseudocyst infection/rupture, biliary stricture with cholangitis, pseudoaneurysm hemorrhage, severe malnutrition)
The Crime Scene: Complications
Now that we know the sentence, let's investigate the full extent of the damage. These are the complications that can escalate the case from misdemeanor to felony.
1) Organ Failure — occurs in ~20% of all acute cases
In the ED, it is important to recognize which patients are most likely to develop organ failure. Risk factors include age ≥ 60 years, significant comorbid disease (heart disease, renal disease, and liver disease), obesity (BMI >30), and heavy alcohol use. Early clinical markers that predict organ failure include the presence of SIRS at admission, elevated or rising BUN and hematocrit (signs of hemoconcentration and hypovolemia), elevated creatinine, and pleural effusions on chest imaging. Patients with these features warrant closer monitoring and more aggressive early resuscitation.
a) Respiratory failure / ARDS — most common organ failure
Pancreatic enzyme activation and systemic inflammation increase pulmonary vascular permeability
b) Acute kidney injury — BUN and Cr are early warning signs
Early: prerenal from hypovolemia and third spacing
Late: intrarenal from systemic inflammation
c) Distributive shock — rising HCT/hemoconcentration is an early marker
Hypotension unresponsive to fluids from massive fluid sequestration and capillary leak
d) Disseminated intravascular coagulation (DIC)
Activation of the coagulation cascade from systemic inflammation leads to consumptive coagulopathy and hemorrhage
2) Local Complications
Approximately 90–95% of acute pancreatitis cases are interstitial edematous pancreatitis, while the remaining 5–10% are necrotizing pancreatitis. The type and frequency of local complications depend on which subtype is present:
a) Interstitial edematous acute pancreatitis (90-95% of acute pancreatitis cases):

pancreatic pseudocyst. original image from local case.
Acute peripancreatic fluid collection (≤4 weeks) — occurs in ~30–40% of all acute pancreatitis patients; usually resolves spontaneously (~70% resolve without intervention)
Pseudocyst (>4 weeks) — encapsulated fluid, no solid component; rare after acute pancreatitis (~6% of cases), as many collections previously labeled pseudocysts are now reclassified as walled-off necrosis
b) Necrotizing acute pancreatitis (5-10% of acute pancreatitis cases):
Acute necrotic collection (≤4 weeks) — heterogeneous fluid + solid debris; develops in ~93% of patients with necrotizing AP
Walled-off necrosis (>4 weeks) — encapsulated mixed solid/fluid; ~59% of acute necrotic collections progress to walled-off necrosis
Infected pancreatic necrosis (typically 2–4 weeks) — gas within necrotic collection on CT scan; occurs in 20–40% of patients with necrotizing AP and carries 15–35% mortality
Requires intervention (percutaneous drainage, endoscopic necrosectomy, or surgery)
3) Vascular Complications
a) Splanchnic venous thrombosis — clot in portal, splenic, or superior mesenteric veins
Occurs in 13–17% of all AP cases overall, increasing to ~24–27% in severe disease
Managed conservatively
Can cause portal hypertension → esophageal/gastric varices
b) Pseudoaneurysm formation and rupture
Pancreatic enzymes erode adjacent arteries (splenic, gastroduodenal, pancreaticoduodenal) forming pseudoaneurysms susceptible to rupture
Typically require emergent angiographic coiling
4) Other Complications
Abdominal compartment syndrome — sustained intra-abdominal pressure >20 mmHg with associated organ failure → requires surgical decompression
Ileus/bowel obstruction — decreased intestinal motility from intra-abdominal inflammation
Pancreatic ascites — from ductal disruption or portal hypertension
GI bleeding — from pseudoaneurysm rupture, variceal bleeding, or stress-related mucosal disease
Interrogation room: ED treatment
The sentence has been handed down and the crime scene fully processed — now it's time to intervene. Treatment intensity should match the severity classification determined above.
Acute Pancreatitis
1. Early IV Fluid Resuscitation
LR > NS (LR associated with decreased SIRS; OR 0.38)
5–10 mL/kg/hr titrated to HR 120, MAP 65–85, UOP 0.5–1 mL/kg/hr, HCT 35–44%
Aggressive hydration most beneficial in the first 6–12 hours
Proceed with caution in CHF and ESRD patients due to risk of pulmonary edema, ARDS, and abdominal compartment syndrome
2. Adequate Pain Control
No single agent has demonstrated superiority
Consider multimodal pain regimen in addition to indicated narcotics
Opioids are NOT contraindicated
3. Early Oral Feeding Within 24 Hours
Low-fat solid diet once pain is improving (think: lean proteins, refined grains, cooked vegetables, low-fat dairy, and fruits instead of fried or greasy foods, full-fat dairy, red meat, butter/oils, nuts, avocado, and rich sauces)
If oral intake is not tolerated, enteral nutrition (NG/NJ) is strongly preferred over parenteral
4. No Benefit of Prophylactic Antibiotics
Reserve for confirmed cholangitis, infected necrosis, or pneumonia
Multiple double-blind RCTs and meta-analyses have consistently shown no benefit in preventing infected necrosis
5. ERCP Consultation
ERCP (endoscopic retrograde cholangiopancreatography) is a procedure that uses endoscopy and fluoroscopy to access and treat problems in the bile and pancreatic ducts
Only indicated urgently for concomitant cholangitis (infection of an obstructed biliary system, classically presenting with Charcot's triad: fever, jaundice, and right upper quadrant pain) or progressive cholestasis (worsening obstruction to bile flow, evidenced by rising bilirubin, alkaline phosphatase, and/or bile duct dilation on imaging)
No improved outcomes outside of that indication for acute pancreatitis
6. Cholecystectomy Timing
Mild biliary AP → same-admission cholecystectomy (ideally within 48 hours) reduces recurrence from 18% to ~0%
Severe or necrotizing → delay cholecystectomy ≥6 weeks
Chronic Pancreatitis
Start with non-opioid analgesics; verify home regimen before escalating
Assess for acute-on-chronic complications (see complications section above)
Consider dose-adjustment and outpatient GI follow-up for patients on pancreatic enzyme replacement therapy (PERT) who present with steatorrhea, malnutrition, or weight loss.
PERT is typically initiated and managed by gastroenterology, not the ED, but it is important to recognize when a patient is on it and whether their symptoms suggest inadequate dosing.
Common FDA-approved PERT products include Creon, Zenpep, Pancreaze, and Pertzye — all porcine-derived formulations dosed by lipase units (typical adult dose: 40,000–50,000 units of lipase per meal, half that with snacks).
If a chronic pancreatitis patient presents with worsening steatorrhea or weight loss despite PERT, ensure adherence and refer to GI for dose titration. The most well-established adjunct is a proton pump inhibitor.
Be careful with insulin administration and glucose timing in patients with pancreatitis-induced diabetes (type 3c) — high risk for hypoglycemia due to concurrent glucagon deficiency.
Type 3c diabetes is diagnosed when new-onset diabetes develops in the setting of (1) pancreatic exocrine insufficiency (e.g., low fecal elastase), (2) pathological pancreatic imaging, and (3) absence of type 1 diabetes autoantibodies.
In practice, any patient who develops diabetes after a diagnosis of chronic pancreatitis should be suspected of having type 3c diabetes.
This is typically confirmed by endocrinology or gastroenterology, but as emergency providers, we should be aware that these patients are uniquely prone to brittle glycemic control because they lack both insulin and glucagon.
Reinforce alcohol and tobacco cessation as these accelerate disease progression
Common ED PITFALLS
| Pitfall | Evidence-Based Approach |
|---|---|
| Giving prophylactic antibiotics | No benefit at any severity; reserve for confirmed infection |
| Ordering routine early ERCP for biliary AP | Only indicated with cholangitis or progressive cholestasis |
| Aggressive unmonitored IV fluids | Goal-directed resuscitation; excessive fluids cause harm |
| Withholding opioids for pain | Opioids are not contraindicated in AP |
| Keeping patient NPO until pain-free | Early oral feeding (within 24h) is recommended |
| Discharging mild biliary AP without surgical plan | Same-admission cholecystectomy prevents recurrence |
Case closed
Pancreatitis is a high-volume, high-acuity diagnosis in the ED. The key takeaways: identify the etiology early (ultrasound for gallstones, lipid panel, medication review), stratify severity to determine the appropriate level of care, resuscitate with goal-directed LR, feed early, avoid prophylactic antibiotics, and watch for complications. For the ~80% with mild disease, some can be safely observed and discharged. For the 20% with organ failure, early recognition and aggressive supportive care save lives.
POST BY: Alexander Landry
Dr. Landry is a PGY-1 in Emergency Medicine at the University of Cincinnati
EDITING BY: ANITA GOEL, MD
Dr. Anita Goel is an APD in Emergency Medicine at the University of Cincinnati and Co-editor of Tamingthesru.com
REFERENCES
1. Garg SK, Sarvepalli S, Campbell JP, et al. Incidence, Admission Rates, and Predictors, and Economic Burden of Adult Emergency Visits for Acute Pancreatitis: Data From the National Emergency Department Sample, 2006 to 2012. J Clin Gastroenterol. 2019;53(3):220-225.
2. Banks PA, Bollen TL, Dervenis C, et al. Classification of Acute Pancreatitis — 2012: Revision of the Atlanta Classification and Definitions by International Consensus. Gut. 2013;62(1):102-111.
3. Mederos MA, Reber HA, Girgis MD. Acute Pancreatitis: A Review. JAMA. 2021;325(4):382-390.
4. Tenner S, Vege SS, Sheth SG, et al. American College of Gastroenterology Guidelines: Management of Acute Pancreatitis. Am J Gastroenterol. 2024;119(3):419-437.
5. Forsmark CE, Vege SS, Wilcox CM. Acute Pancreatitis. N Engl J Med. 2016;375(20):1972-1981.
6. Boxhoorn L, Voermans RP, Bouwense SA, et al. Acute Pancreatitis. Lancet. 2020;396(10252):726-734.
7. Beyer G, Habtezion A, Werner J, Lerch MM, Mayerle J. Chronic Pancreatitis. Lancet. 2020;396(10249):499-512.
8. Singh VK, Yadav D, Garg PK. Diagnosis and Management of Chronic Pancreatitis: A Review. JAMA. 2019;322(24):2422-2434.
9. Bálint ER, Fűr G, Kiss L, et al. Assessment of the Course of Acute Pancreatitis in the Light of Aetiology: A Systematic Review and Meta-Analysis. Sci Rep. 2020;10(1):17936.
10. Waller A, Long B, Koyfman A, Gottlieb M. Acute Pancreatitis: Updates for Emergency Clinicians. J Emerg Med. 2018;55(6):769-779.
11. Lankisch PG, Weber-Dany B, Hebel K, Maisonneuve P, Lowenfels AB. The Harmless Acute Pancreatitis Score: A Clinical Algorithm for Rapid Initial Stratification of Nonsevere Disease. Clin Gastroenterol Hepatol. 2009;7(6):702-705.
12. Maisonneuve P, Lowenfels AB, Lankisch PG. The Harmless Acute Pancreatitis Score (HAPS) Identifies Non-Severe Patients: A Systematic Review and Meta-Analysis. Pancreatology. 2021;21(8):1419-1427.
13. Kuo DC, Rider AC, Estrada P, Kim D, Pillow MT. Acute Pancreatitis: What's the Score? J Emerg Med. 2015;48(6):762-770.
14. Anderson K, Shah I, Yakah W, et al. Prospective Evaluation of an Emergency Department Protocol to Prevent Hospitalization in Mild Acute Pancreatitis: Outcomes and Predictors of Discharge. Pancreatology. 2023;23(3):299-305.
15. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A New Method of Classifying Prognostic Comorbidity in Longitudinal Studies: Development and Validation. J Chronic Dis. 1987;40(5):373-383.
16. Szakács Z, Gede N, Pécsi D, et al. Aging and Comorbidities in Acute Pancreatitis II: A Cohort-Analysis of 1203 Prospectively Collected Cases. Front Physiol. 2019;10:420.
17. Hidalgo NJ, Pando E, Mata R, et al. Impact of Comorbidities on Hospital Mortality in Patients With Acute Pancreatitis: A Population-Based Study of 110,021 Patients. BMC Gastroenterol. 2023;23:91.
18. Lee PJ, Lahooti A, Culp S, et al. Obesity and Alcoholic Etiology as Risk Factors for Multisystem Organ Failure in Acute Pancreatitis: Multinational Study. United European Gastroenterol J. 2023;11(4):385-393.
19. Trout AT, Anupindi SA, Freeman AJ, et al. NASPGHAN/SPR Joint Position Paper on Noninvasive Imaging of Pediatric Pancreatitis. J Pediatr Gastroenterol Nutr. 2021;72(1):151-167.
20. Mehta MS. Acute Pancreatitis in Children: Risk Factors, Management, and Outcomes. Curr Opin Pediatr. 2023;35(5):590-595.
21. McNabb-Baltar J, Suleiman SL, Banks PA, Conwell DL. Outcomes of Chronic Pancreatitis in the Emergency Department. Dig Dis Sci. 2018;63(11):2874-2879.
22. Garg PK, Singh VP. Organ Failure Due to Systemic Injury in Acute Pancreatitis. Gastroenterology. 2019;156(7):2008-2023.
23. Komara NL, Paragomi P, Greer PJ, et al. Severe Acute Pancreatitis: Capillary Permeability Model Linking Systemic Inflammation to Multiorgan Failure. Am J Physiol Gastrointest Liver Physiol. 2020;319(5):G573-G583.
24. Moggia E, Koti R, Belgaumkar AP, et al. Pharmacological Interventions for Acute Pancreatitis. Cochrane Database Syst Rev. 2017;4:CD011384.
25. Manrai M, Kochhar R, Gupta V, et al. Outcome of Acute Pancreatic and Peripancreatic Collections Occurring in Patients With Acute Pancreatitis. Ann Surg. 2018;267(2):357-363.
26. Muthusamy VR, Chandrasekhara V, Acosta RD, et al. The Role of Endoscopy in the Diagnosis and Treatment of Inflammatory Pancreatic Fluid Collections. Gastrointest Endosc. 2016;83(3):481-488.
27. Leppäniemi A, Tolonen M, Tarasconi A, et al. 2019 WSES Guidelines for the Management of Severe Acute Pancreatitis. World J Emerg Surg. 2019;14:27.
28. Szatmary P, Grammatikopoulos T, Cai W, et al. Acute Pancreatitis: Diagnosis and Treatment. Drugs. 2022;82(12):1251-1276.
29. Borbély RZ, Szalai EÁ, Philip BM, et al. The Risk of Developing Splanchnic Vein Thrombosis in Acute Pancreatitis Increases 3 Days After Symptom Onset: A Systematic Review and Meta-Analysis. United European Gastroenterol J. 2024;12(6):735-746.
30. Anis FS, Adiamah A, Lobo DN, Sanyal S. Incidence and Treatment of Splanchnic Vein Thrombosis in Patients With Acute Pancreatitis: A Systematic Review and Meta-Analysis. J Gastroenterol Hepatol. 2022;37(3):462-472.
31. Crockett SD, Wani S, Gardner TB, Falck-Ytter Y, Barkun AN. American Gastroenterological Association Institute Guideline on Initial Management of Acute Pancreatitis. Gastroenterology. 2018;154(4):1096-1101.
32. Hong J, Li Q, Wang Y, et al. Comparison of Fluid Resuscitation With Lactate Ringer's Versus Normal Saline in Acute Pancreatitis: An Updated Meta-Analysis. Dig Dis Sci. 2024;69(1):282-293.
33. Oppenlander KE, Chadwick C, Carman K. Acute Pancreatitis: Rapid Evidence Review. Am Fam Physician. 2022;106(1):44-50.
34. An Z, Braseth AL, Sahar N. Acute Cholangitis: Causes, Diagnosis, and Management. Gastroenterol Clin North Am. 2021;50(2):403-414.
35. Whitcomb DC, Buchner AM, Forsmark CE. AGA Clinical Practice Update on the Epidemiology, Evaluation, and Management of Exocrine Pancreatic Insufficiency: Expert Review. Gastroenterology. 2023;165(5):1292-1310.
36. Ramsey ML, Forsmark CE. Exocrine Pancreatic Insufficiency. JAMA. 2026.
37. U.S. Food and Drug Administration. Creon (pancrelipase) Prescribing Information. 2024.
38. American Diabetes Association. Diagnosis and Classification of Diabetes: Standards of Care in Diabetes — 2026. Diabetes Care. 2026;49(Suppl 1).
39. Johnston PC, Thompson J, McKee A, et al. Diabetes and Chronic Pancreatitis: Considerations in the Holistic Management of an Often Neglected Disease. J Diabetes Res. 2019;2019:2487804.
40. Nagy R, Ocskay K, Sipos Z, et al. Discharge Protocol in Acute Pancreatitis: An International Survey and Cohort Analysis. Sci Rep. 2023;13(1):22109.
41. Sartelli M, Chichom-Mefire A, Labricciosa FM, et al. The Management of Intra-Abdominal Infections From a Global Perspective: 2017 WSES Guidelines. World J Emerg Surg. 2017;12:29.
42. Baron TH, DiMaio CJ, Wang AY, Morgan KA. American Gastroenterological Association Clinical Practice Update: Management of Pancreatic Necrosis. Gastroenterology. 2020;158(1):67-75.e1.




{kind=link}
{kind=link}