Interpreting Elbow and Forearm Radiographs
/Elbow injuries account for 2-3% of all emergency department visits across the nation (1). Yet, because of the elbow’s complex anatomy and the presence of numerous ossification centers in children, elbow fractures are the third most commonly missed fracture group in the ED (1). Here are some tools to help ED physicians read elbow x-rays more effectively and hopefully identify abnormalities more easily.
Elbow Anatomy

Normal Ossification Centers of the Elbow
We all know the basic anatomy of the elbow with the humerus, radius, and ulna. However, as emergency physicians it is important to recognize the elbow ossification centers that develop during childhood in order to accurately interpret radiographs of the joint. These ossification centers can be mistaken for fractures if one is not careful. There are six ossification centers which develop in a predictable order at somewhat predictable ages. The mnemonic for this is CRITOE.
The Capitellum is first, then the Radial head, followed by the Internal or medial epicondyle. T is for Trochlea, then Olecranon, and E is for the External or lateral epicondyle.
There are normal age ranges during which these will develop, and girls often develop them at slightly younger ages than boys, usually 6-12 months ahead of their male counterparts. In general, an ossification center develops approximately every two years starting with the capitellum around the age of two. Nonetheless, knowledge of the order in which these develop is really what is crucial to help identify fractures from normal ossification centers.
Radiographic Pearls
Alignment
When reviewing imaging of the elbow, one should look for appropriate joint alignment. This involves evaluating two specific markers of alignment. The first is the anterior humeral line. An imaginary line drawn along the front of the humerus should intersect the middle to anterior third of the capitellum. If it does not, a supracondylar fracture should be suspected.

Normal Alignment on a Lateral Elbow Radiograph

Supracondylar Fracture (note that the anterior humeral line does not intersect the capitellum)
The next marker of a normal elbow x-ray is the radiocapitellar line. A line drawn through the middle of the radius should pass through the middle of the capitellum. If it does not, radial head dislocation is likely present.

Radial Head Dislocation (radiocapitellar line does not intersect capitellum)
Fat Pads
On a normal elbow x-ray, only a small stripe of an anterior fat pad should be visible. No posterior fat pad should be seen. Injuries around the joint can produce a joint effusion which will displace the fat pads making them more visible. The anterior fat pad protrudes more and looks pointy; this is what is recognized as the sail sign. The posterior fat pad can be visualized as well in the presence of effusion, and if seen is always abnormal.

Sail Sign and Posterior Fat Pad
Common Elbow Injuries
Pediatrics
Supracondylar Fracture: The most common elbow fracture in pediatrics is a supracondylar fracture, making up to 60% of pediatric elbow fractures2. Things to look for would be malalignment of the anterior humeral line as mentioned above. Additionally, the presence of the sail sign and posterior fat pad should prompt further evaluation of the image.
Lateral Condyle Fracture: 15-20% of pediatric elbow fractures are lateral condyle fractures (2). Identification of this requires knowledge of the ossification centers and identification of what should be present versus what is abnormal.
Medial Epicondyle Fracture: 5-10% of pediatric elbow fractures are medial epicondyle fractures (2). An important mechanism for developing this is elbow dislocation during which the medial epicondyle can be avulsed. During reduction, that small epicondyle can actually get stuck in the joint capsule and can easily be overlooked when reading an x-ray. Be aware of this and look for it on post-reduction films.

Supracondylar Fracture

Lateral Condyle Fracture

Medial Epicondyle Fracture
Adults
Radial Head Fracture: Up to 50% of elbow fractures in adults are of the radial head making it the most common elbow injury in adults (3). Overwhelmingly, it is also the most commonly missed elbow fracture. Therefore, take a very close look at the radial head, particularly when evaluating adult elbow films.
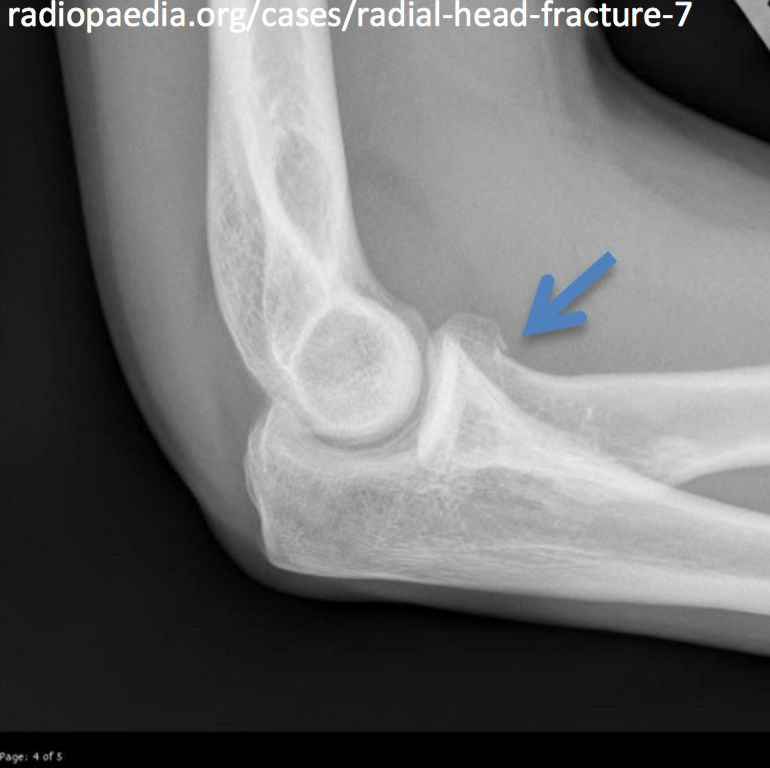
Radial Head Fracture
Common Forearm Fractures
Forearm fractures are the most common fractures seen in pediatrics and account for 31% of all adult upper extremity complaints (4). In general, identification of these fractures is less complex than the elbow. However, there are two important fracture classifications that are commonly tested on examinations. A mnemonic to help remember this is MUGR meaning Monteggia- ulna, Galeazzi- radius.
Monteggia Fracture: This is a proximal ulnar fracture with a radial head dislocation. If there is malalignment of the radiocapitellar line, it is important to image the forearm and evaluate for ulnar fracture as these commonly go hand-in-hand.
Galeazzi Fracture: This is a distal radius fracture with dislocation of the ulna. Here, the wrist needs to be imaged in addition to the forearm.
References
- Blumberg S, Kunkov S, Crain E, et al. The predictive value of a normal anterior fat pad sign following elbow trauma in children. Pediatric Emergency Care, 2011. 7: 596-600.
- Skaggs D, Mirzayan R. The posterior fat pad sign in association with occult fracture of the elbow in children. American Journal of Bone and Joint Surgery, 1999. 10: 1429-33
- Pavic R, Margetic P, Hnatesen D. Diagnosis of occult radial head and neck fractures in adults.Injury, 2015. 46: 119-24.
- Slaar A, Walenkamp M, Bentohami A, et al. A clinical decision rule for the use of plain radiography in children after acute wrist injury: development and external validation of the Amsterdam Pediatric Wrist Rules. Pediatric Radiology, 2016. 46:50-60.
Written by Jessica Merriam, MD, PGY-1 Resident at the University of CIncinnati Department of Emergency Medicine
Edited and Posted by Dr. Jeffery Hill, MD MEd



