HIV in the ED: The 3 AM Questions You Actually Care About
/HIV shows up in the ED in more ways than we realize — from needle sticks to acute retroviral syndrome to the patient who quietly screens positive on routine labs. And at 3 am, the questions that matter aren’t abstract pathophysiology but the practical ones: When do I start PEP? How do I not miss acute HIV? Should I really be starting treatment from the ED? Join Dr. Hoeflinger as she breaks down what every emergency physician needs to know to diagnose, treat, and counsel patients with confidence through 10 FAQs about HIV.
1) What do I need to remember about HIV pathophysiology when I’m staring at a CBC at 3 am?
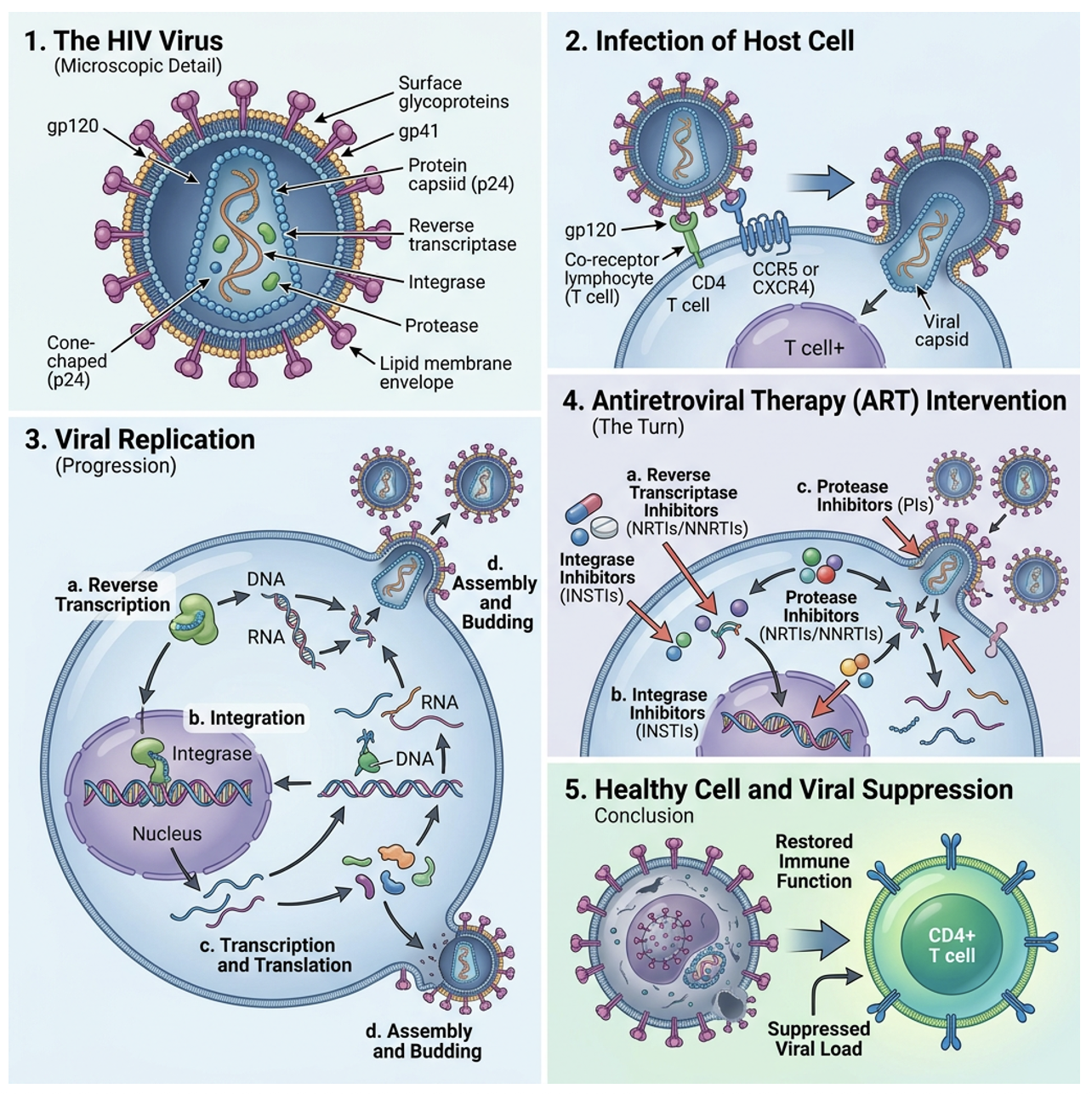
Image from https://easy-peasy.ai/ai-image-generator/images/hiv-journey-antiretroviral-therapy-success (AI generated). Free to use under no copyright with link above. Accessed may 20, 2026.
Often early HIV can be seen on an initial CBC with mild leukopenia, or advanced HIV can be seen with lymphopenia, but neither of these are very specific. This is because HIV is a retrovirus that primarily targets CD4 T‑helper lymphocytes, leading to progressive destruction of cell‑mediated immunity and increased susceptibility to opportunistic infections. This means that to know the status of an HIV patient’s immune system, physicians really need to know the most recent CD-4 count.
Before antiretroviral therapy for HIV was created in the 1990s, because of the slow destruction of the immune system as described above, HIV/AIDS was essentially always fatal over time. However, advances in anti‑Retroviral Therapy (ART) in the last twenty years have transformed HIV into a chronic disease with near‑normal life expectancy for patients maintaining treatment adherence.
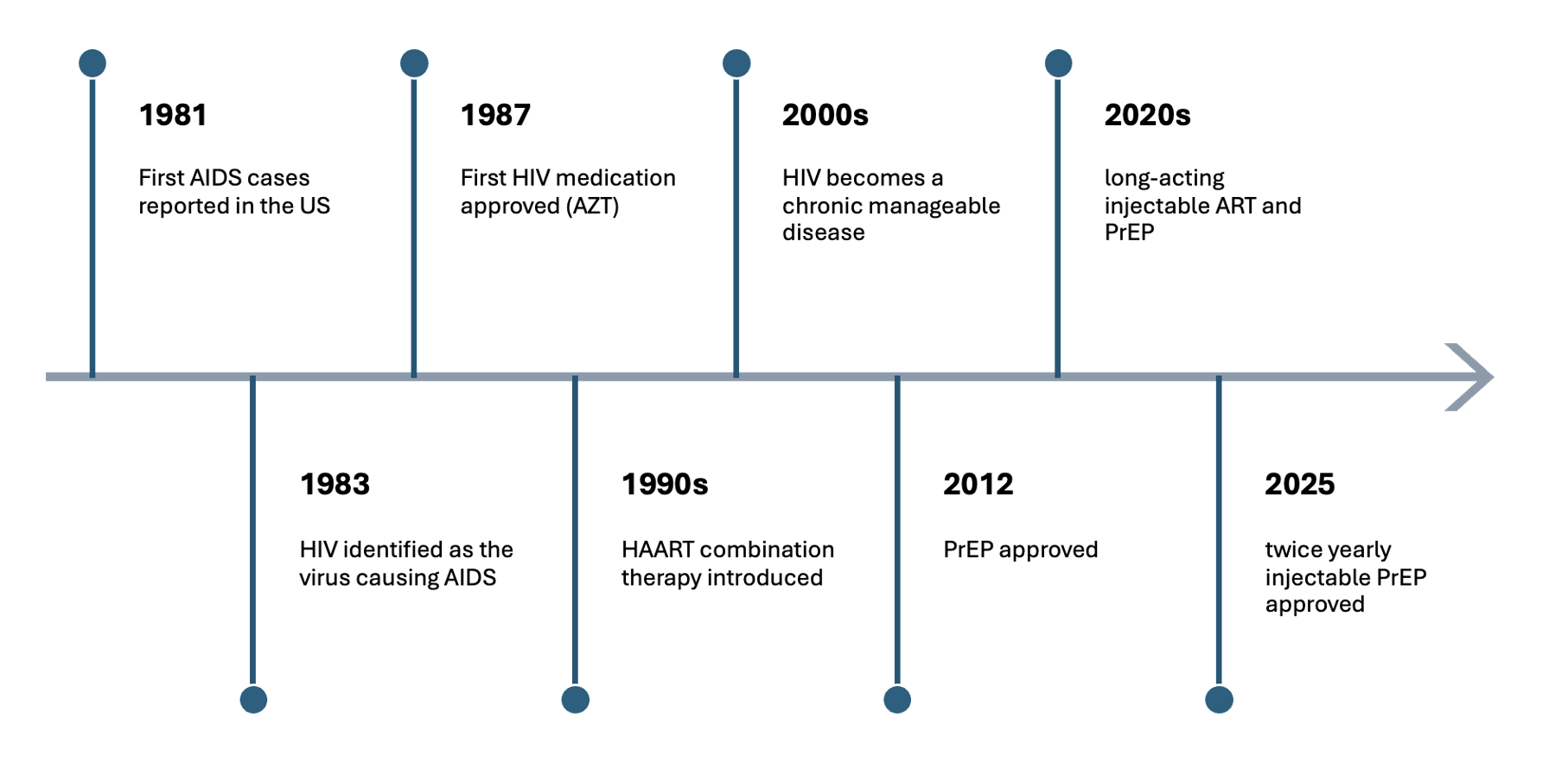
“a timeline of HIV from identification to present” — original image created from references linked at bottom of page
2) How common is HIV in the U.S., Ohio, and Cincinnati? Should I be thinking about it more often?
U.S. (2023): 1.13 million people living with diagnosed HIV
Undiagnosed HIV: ~153,500 people (≈15% of all people living with HIV)
Ohio: 25,241
Hamilton County: 3,198 (rate 451/100,000 — nearly double the state average)
Translation: Yes – think about HIV. A lot of patients seen in the ED may have either diagnosed or undiagnosed HIV.
3) What HIV‑related presentations am I most likely to see in the ED?
New diagnosis after screening or symptomatic testing
Patients requesting PEP
Patients seeking or needing PrEP
Acute HIV viral syndrome
IRIS after ART initiation
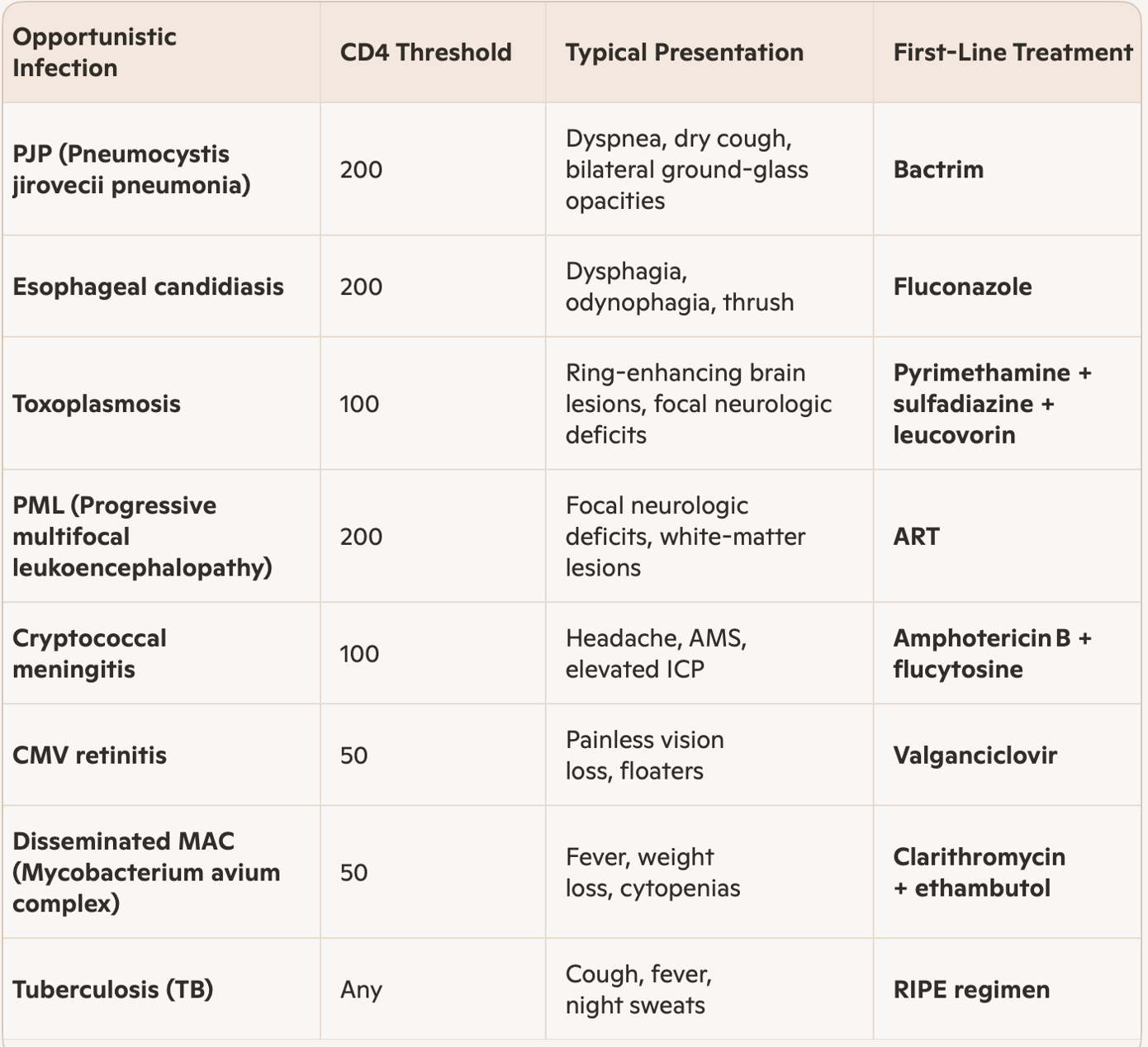
AIDS‑defining illnesses in advanced disease
4) What is PEP, when should I start it, and what does the CDC say in 2025?
PEP is post‑exposure prophylaxis — short‑term antiretroviral treatment given after a potential HIV exposure to prevent seroconversion.
Common exposures include:
Sexual assault
Needlestick exposure (usually healthcare workplace–related accidental injury)
Condomless sex with HIV‑positive or unknown‑status partner
Needle sharing
Per the 2025 CDC PEP guidelines, ED physicians can and should initiate PEP without requiring ID consultation.
The first dose should be given as soon as possible, ideally within 24 hours, and no later than 72 hours.
Recommended regimens:
Non‑pregnant patients: 28 days of Biktarvy (bictegravir/emtricitabine/tenofovir alafenamide 50‑200‑25 mg)
Pregnant patients: 28 days of Tivicay (dolutegravir 50 mg) + Descovy (emtricitabine/tenofovir alafenamide 200‑25 mg)
Baseline labs:
Rapid HIV test
Pregnancy test (if applicable)
Hepatic function panel
Basic metabolic panel
Completion rates are very low (11–15%) when the course is not started in the ED and fully dispensed up front. Protocols that provide the first dose and the full course before discharge dramatically improve adherence.
5) What is PrEP, what are current options, and what new options may be ready in the near future for use?
PrEP is medication taken by HIV‑negative individuals (who may frequently partake in high risk behaviors) to prevent HIV infection.
Studies show a significant risk reduction with use of PrEP:
~99% for sexual transmission
≥74% for injection drug use
Current FDA‑approved daily pills:
Truvada (emtricitabine and tenofovir disoproxil fumarate)
Descovy (emtricitabine and tenofovir alafenamide)
Newer options:
Apretude — monthly injectable cabotegravir (FDA 2021)
Lenacapavir (Yetzugo) — twice‑yearly injectable (FDA 2025)
In development:
Intravaginal rings
Implants
Broadly neutralizing antibodies
6) How do I not miss acute HIV in the ED — and why is it so easy to miss?
Acute HIV typically presents 2–6 weeks after exposure with a nonspecific viral syndrome that looks like flu, mono, or any other regular viral illness — and if an ED physician doesn’t think about it, they may miss it.
Common symptoms:
Fever (~93%)
Fatigue/malaise
Maculopapular rash
Pharyngitis
Lymphadenopathy
Headache
Myalgias/arthralgias
Diarrhea
Oral ulcers
Night sweats
Labs: leukopenia, thrombocytopenia, transaminitis.
If suspicion is high and the Ag/Ab test is negative → order HIV‑1 RNA.
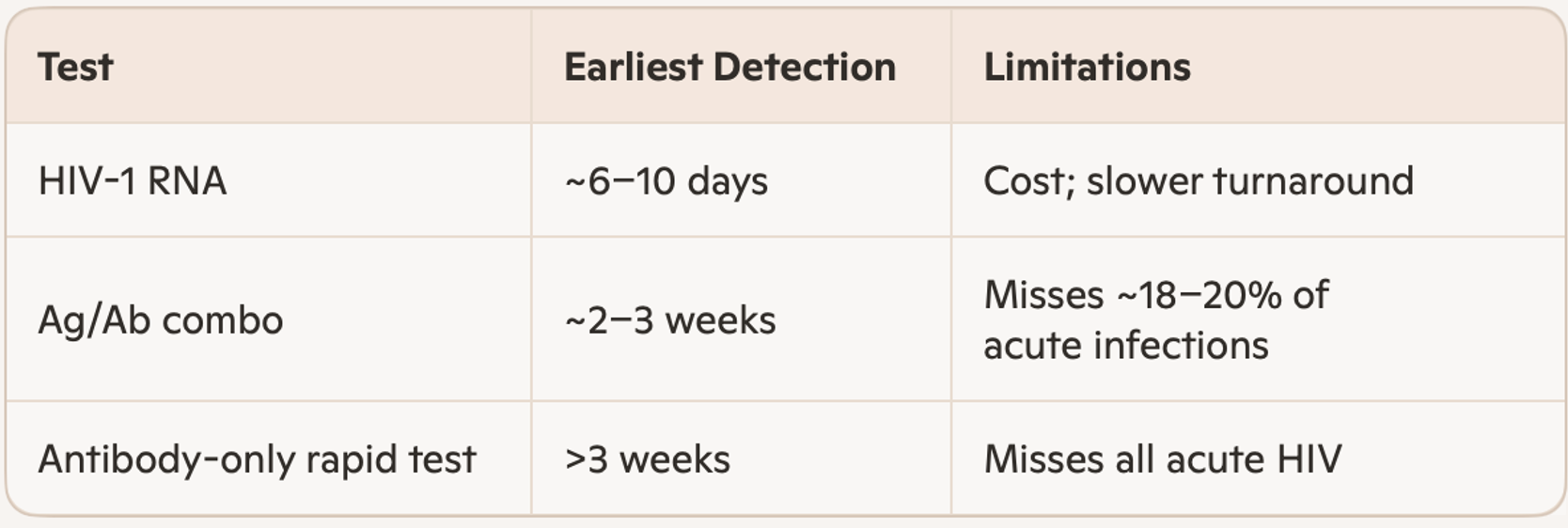
original table created from references below.
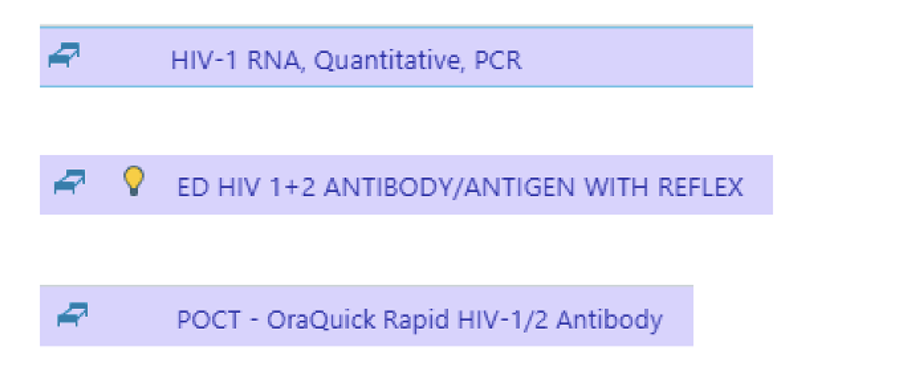
At our institution (UCMC) these tests look like the following in Epic (in order 1-3 as above in table):
7) What Ohio‑specific rules do I need to remember about HIV testing?
Ohio requires notification with opt‑out testing. Suggested phrasing:
“Part of your workup today includes HIV testing. You can decline this test if you do not want it.”
8) How do I tell someone they might have (or do have) HIV? It feels like a high‑stigma diagnosis, and patients may panic — how do I do this well?
Deliver the result directly, calmly, and without euphemisms, while recognizing the emotional weight and stigma patients may carry.
Key elements:
“Your HIV test was positive.”
(Even though confirmation is pending, it is extremely likely they are infected, so counsel accordingly.)
HIV is a virus that attacks the immune system.
HIV is treatable with proper medical care and follow‑up, though not curable.
A member of the ED staff will contact them with confirmed results.
Allow silence. Let them process. Avoid overwhelming them with details in the first conversation.
9) Should I start anti-retroviral therapy (ART) in the ED?
All major guidelines (NIH/OARAC, IAS‑USA, and HIVMA/IDSA) recommend same‑day or rapid ART initiation (within 7 days of diagnosis). The NIH guidelines state that ART does not need to be delayed while awaiting confirmatory testing or resistance results.
There was a recent quality improvement study conducted from 2021–2022 at an ED with 70,000 visits/year that aimed to connect patients with a starter pack of ART from the ED immediately after HIV diagnosis, hoping it would decrease barriers to care and improve outcomes.
Inclusion criteria were:
Not currently pregnant
Were unlikely to have a false‑positive Ag/Ab test result
Were planned to discharge home
ART‑naïve
Acceptable liver and renal function
Lacked symptoms of an opportunistic infection
Judged to be a good candidate
Outcomes:
Patients who received ED‑initiated rapid ART demonstrated significantly higher 30‑day follow‑up rates (82.6% vs 50.0%).
The 6‑month incidence of immune reconstitution inflammatory syndrome (IRIS) — an exaggerated inflammatory response that occurs when the immune system begins to recover after ART initiation — was 4.3% among the 23 patients who were HIV‑positive and receiving ED rapid ART.
10) What is IRIS, how do I recognize it, and what do I do about it?
Immune reconstitution inflammatory syndrome (IRIS) occurs after ART initiation when the recovering immune system triggers an exaggerated inflammatory response to an existing opportunistic infection. In the ED, think of IRIS in a patient recently started on ART who appears clinically worse despite improving HIV treatment adherence. IRIS is a clinical diagnosis with no specific laboratory test for confirmation, making it a diagnosis of exclusion.
IRIS occurs in an estimated 10–30% of patients starting ART with advanced immunosuppression (very low baseline CD4 count/high baseline HIV RNA), typically within the first weeks to months.
Things that can point to IRIS:
Close association of symptoms beginning with ART initiation (typically within 1 week to 3 months)
Evidence of immune system restoration (rising CD4 count, declining viral load)
Negative infectious workup in a patient with signs of improving cellular immunity
High‑risk patients: baseline CD4 <50–100 and short interval between opportunistic infection treatment and ART initiation
Types of IRIS:
Paradoxical IRIS: Worsening of a known, treated opportunistic infection after ART initiation
Unmasking IRIS: A previously subclinical opportunistic infection becomes clinically apparent after ART‑driven immune recovery
Management:
From an ED perspective, these patients should be admitted for further workup to help differentiate IRIS from active opportunistic infection, as infectious cultures and viral loads/CD4 counts will still be pending.
Continue ART and treat the underlying infection — do not stop ART unless life‑threatening
Mild cases: symptomatic management
Moderate‑to‑severe cases: consider steroids
original table created from references below.
Summary
HIV intersects with emergency medicine in ways that are both common and often under‑recognized. ED clinicians play a critical role in preventing new infections through timely PEP and PrEP initiation, identifying acute HIV that masquerades as routine viral illness, navigating Ohio’s opt‑out testing laws, delivering difficult diagnoses with clarity and compassion, and even starting ART directly from the ED. Understanding IRIS, recognizing high‑risk presentations, and staying current with evolving prevention and treatment options allows emergency physicians to meaningfully impact patient outcomes — even at 3 am.
Post by: nICOLE hOEFLINGER
Dr. Hoeflinger is a PGY-1 in Emergency Medicine at the University of Cincinnati
Editing by: Anita Goel, MD
Dr. Anita Goel is an APD in Emergency Medicine at the University of Cincinnati and Co-editor of Tamingthesru.com
References
HIV.gov. HIV and AIDS timeline. HIV.gov. https://www.hiv.gov/hiv-basics/overview/history/hiv-and-aids-timeline.
AIDSVu. HIV prevalence in the United States. AIDSVu. https://map.aidsvu.org/.
Saag MS. HIV infection—screening, diagnosis, and treatment. N Engl J Med. 2024;390(3):239-251. doi:10.1056/NEJMcp1915826.
Tanner MR, et al. Antiretroviral postexposure prophylaxis after sexual, injection drug use, or other nonoccupational exposure to HIV—CDC recommendations, United States, 2025. MMWR Recomm Rep. 2025;74(1):1-56. doi:10.15585/mmwr.rr7401a1.
Gandhi M, et al. Long-acting injectable antiretroviral therapy for HIV treatment and prevention. JAMA. 2023;329(2):157-168. doi:10.1001/jama.2022.24500.
HIV.gov. Long-acting PrEP. HIV.gov. https://www.hiv.gov/hiv-basics/hiv-prevention/potential-future-options/long-acting-prep.
Kahn JO, Walker BD. Acute human immunodeficiency virus type 1 infection. N Engl J Med. 1998;339(1):33-39. doi:10.1056/NEJM199807023390107.
Branson BM, Owen SM, Wesolowski LG, et al. Laboratory testing for the diagnosis of HIV infection: updated recommendations. JAMA. Published online 2016. https://jamanetwork.com/journals/jama/fullarticle/2491636.
Panel on Antiretroviral Guidelines for Adults and Adolescents. Guidelines for the use of antiretroviral agents in adults and adolescents with HIV. Clinicalinfo.HIV.gov. https://clinicalinfo.hiv.gov/sites/default/files/guidelines/documents/adult-adolescent-arv/guidelines-adult-adolescent-arv.pdf.
Ohio Rev Code §3701.242. Informed consent to HIV test required. https://codes.ohio.gov/ohio-revised-code/section-3701.242.
MD checklist: counseling patients with preliminary positive HIV test results. https://static1.squarespace.com/static/53c1a2cce4b0e88e61f99b70/t/559d29d0e4b08185b195f63f/1436363216264/MD+Checklist+Post-test+Counsel+for+Prelim+Pos+2012+05-29.pdf.
Panel on Antiretroviral Guidelines for Adults and Adolescents. Guidelines for the use of antiretroviral agents in adults and adolescents with HIV. Clinicalinfo.HIV.gov. https://clinicalinfo.hiv.gov/sites/default/files/guidelines/documents/adult-adolescent-arv/guidelines-adult-adolescent-arv.pdf.
White D, Jewett M, Burns M, et al. Implementing a rapid antiretroviral therapy program using starter packs for emergency department patients diagnosed with HIV infection. J Clin Virol. 2023;164:105502. doi:10.1016/j.jcv.2023.105502.
Panel on Guidelines for the Prevention and Treatment of Opportunistic Infections in Adults and Adolescents With HIV. Guidelines for the prevention and treatment of opportunistic infections in adults and adolescents with HIV. Clinicalinfo.HIV.gov. https://clinicalinfo.hiv.gov/sites/default/files/guidelines/documents/adult-adolescent-oi/guidelines-adult-adolescent-oi.pdf.
Meintjes G, Scriven J, Marais S. Management of the immune reconstitution inflammatory syndrome. Curr HIV/AIDS Rep. 2012;9(3):238-250. doi:10.1007/s11904-012-0129-5.
Vanderbilt Internal Medicine Residency Handbook. AIDS-defining clinical conditions. https://vimbook.vumc.org/infectious-diseases/aids-defining-clinical-conditions.



