Is There a Doc on Board? Recap and Curated Commentary
/
African Tick Borne Illness
Hypothermic cardiac arrest
We were fortunate, a couple weeks back, to have Dr. Brian Burns of Sydney HEMS come and speak to us. In his lecture, “When the 1% Makes All the Difference” which you can find here, Dr. Burns hit on a number of excellent points. We sat down and talked with Dr. Burns a bit more extensively over a couple of the themes of his lecture.
In this podcast, we cover some of the plus/minuses of checklists, the importance of high fidelity continuous training practices (simulation, routine case debriefing, intensive induction training), and the role of cognitive factors in running resuscitations.
Should resuscitations run like a jazz quartet or a Formula 1 pit crew? Are checklists simply in the way or do they cognitively unload the team members to improve performance? How do you train cognitive factors in resuscitation?
Read MoreJust prior to SMACC (the Social Media and Critical Care Conference), we were lucky enough to have Dr. Brian Burns of Sydney HEMS stop through Cincinnati. In the video below you can see his lecture on when the 1% makes all the difference. Dr. Burns talks about how we should strive for excellence in prehospital care not simply meeting minimum standards. Watch the lecture below to hear Dr. Burns discuss the importance of incremental changes, cognitive offloading, checklists, and continuous improvement and training through simulation.
Read MoreIn July, the entire emergency department is full of firsts; firsts shift in a new pod, first solo flights, first successful codes, and first shifts supervising new providers. This is an exciting time -- full of new faces and new roles. July can also be scary. All of those new roles come with uncertainty, fear of the unfamiliar, and immense responsibility.
This issue features cases and #lessonslearned from graduates whose “firsts” were not so long ago. These are showcased to serve as a reminder to us all that although this month is full of firsts for the residents, our faculty, nurses, and department have seen many Julys pass and are ready and eager to teach us their own #lessonslearned. Check out the new issue to see!
Keep your presentation simple. Remember that good artists borrow and great artists steal. Find presenters that inspire you.
Know your audience and environment
P3: Prepare, Practice, Pitch
Read MoreThanks to everybody who commented and contributed to the discussion on our final “Flight!” If you missed out on the case, check it out here. Below you’ll find a curation of the comments to each question and a podcast with expert commentary from Jenn Lakeberg, APRN. This was the final “Flight” for this spring/summer. Look for the cases to return again in January 2016 as we begin Flight MD Orientation with the next class of future Air Care Flight Docs.
Read More#lessonslearned is a case series submitted by former senior residents describing B-pod cases that taught them the art of medicine
A male in his 30s with a past medical history significant for hypertension presented via EMS with pain all over, anxiety and shortness of breath. The EMTs reported that he had smoked marijuana about 30 minutes before his presentation from his normal supply. At the scene he was noted to be very agitated, diaphoretic and vocal about his pain. He was yelling that he was hurting all over, he was having trouble breathing, and that he wanted to be sedated. He states that he has never had problems like this.
Read MoreIt's 6pm in the ED on a sunny summer afternoon- you're working as a single coverage physician at a level 3 trauma center. You are noticing an uptrend in the trauma patients being brought in over the past few hours. While log rolling yet another patient, an EMS provider tells you that they have been making runs nonstop- all of the hospitals downtown are overloaded, and it doesn't look like it will slow down anytime soon. Your modest trauma bay is already full, and you're starting to sweat about the state of the department- there are 4 patients in the pod you haven't even seen yet, 2 with abnormal vital signs.
Read MoreYou are a 4th year EM resident moonlighting on your first day in a remote area as the solo provider that has minimal availability to consulting services. The nearest major hospital is approximately 100 miles away.
A 5 year old child enters your ED at 3 am with a large, complex laceration to the face from a dog bite which will likely require sedation and a layered closure. His injuries were sustained approximately 6 hours ago. The wound is complex and will require a multi-layered closure and there are a couple of areas of tissue avulsion. You have 1 or 2 cases of similar experience from approximately 1 year ago on your plastics rotation...
Read MoreYou are an EM resident from the US working in a rural South African hospital as part of a global health elective. The political climate is such that a prolonged government strike is leading to severe staffing and resource shortage. There are no disposable gloves and many procedures are performed barehanded. One day during rounds in the Labor Ward, the Chair of the department asks you to draw blood from an HIV-positive woman in labor as the team is presenting the patient in her room. The only remaining gloves in the hospital are a few pairs of sterile gloves reserved for emergency cesarean deliveries. There are high rates of HIV-exposure and many staff members are currently on post-exposure prophylaxis.
Read MoreYou are enjoying a cocktail on the way to Hawaii on a well earned vacation when a voice comes aloud overhead, “Attention all passengers. If there is a doctor or health care provider present, we ask that you please come to the front of the plane immediately.” From your vantage point in the back of the plane, it becomes clear very quickly that no one is volunteering. You find yourself being stared at by a plane full of people as you make your way to the front, to find a morbidly obese Caucasian female with a flight attendant at her side. You start your encounter…
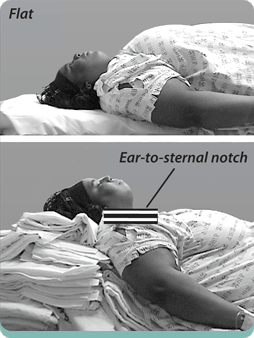
Read MoreMultiple casualties are brought to you from a house fire. There are four victims:
You determine that they all require intubation for various indications. You choose RSI as the method for all except the morbidly obese patient, who you intend to intubate awake, with sedation and topical airway anesthesia.
Question:
How would you position each of these patients to optimize your chances of successful intubation on the first attempt?
Read MoreImagine: you are the single provider manning a rural clinic in Northern Tanzania along the shore of Lake Victoria. You are one of only a handful of physicians in the entire region and you have minimal access to diagnostics or therapeutics. Your clinic does not have any power. Your diagnostics include: urinalysis, urine pregnancy, CBC and rapid tests for HIV, syphilis, and malaria. You have 2 nurses, one of whom acts as a translator (from Swahili to English). You are armed primarily with your intellect, knowledge of local disease processes, and your keen sense of intuition.
Read MoreIf you want to get a group of prehospital providers riled up, simply ask them how the airway should be managed during out-of-hospital cardiac arrest. "Supraglottic airways are easier!" "No, you gotta stay with endotracheal intubation!" "Forget advanced airways, a bag-valve mask is all you need!" "Only apneic oxygenation!" Don't believe me?
Read MoreSRU (pronounced "shrew") = Shock Resuscitation Unit
Training in, and managing, the SRU is one of the crown jewels of our residency. It is where the sickest of the sick patients are found in our ED. It is a crucible, a test of knowledge and strength, and a true manifestation of the tripartite mission of our department: Leadership, Excellence, and Opportunity.
Training in, and managing, the SRU is one of the crown jewels of our residency. It is where the sickest of the sick patients are found in our ED. It is a crucible, a test of knowledge and strength, and a true manifestation of the tripartite mission of our department: Leadership, Excellence, and Opportunity.
Check out AI contexted information from this and other great FOAMed sites via FOAMCortex