Tube Thoracostomy
Indications
- Primary or Secondary Spontaneous Pneumothorax
- Clinical suspicion of tension pneumothorax - Unstable Patients (RR >24 breaths/min, HR <60 bpm or >120 bpm, abnormal BP, room air 02 sat <90%, or cannot speak in full sentences)
- Large Pneumothoraces (>3 cm Apex-to-Cupola Distance -OR- >2 rib spaces at the apex or 2 cm from the lateral chest wall)
- Overt Traumatic Pneumothorax (diagnosed clinically or by CXR)
- Hemothorax
- Empyema
Preparation
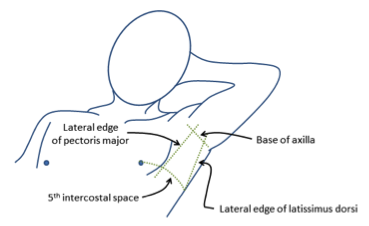
Triangle of Safety - http://www.oxfordmedicaleducation.com/procedures/intercostal-drain/
- Obtain Informed Consent if able including a discussion with the patient about potential complications of the procedure
- Dress – Mask, eye shield, gown, sterile gloves, headwear
- Ensure that the Pleura-vac is set up
- Position Patient
- Head of bed 30 to 45 degrees (unless the patient is in spinal precautions as a result of trauma)
- Using a soft wrist restraint, Secure the arm on the affected side out of the field
- Identify Site of Procedure
- “Triangle of safety” - Lateral edge of the pectoralis major, mid-axillary line, and above the 5th intercostal space (nipple line in males, inframammary crease in females)
- Insertion site should be in the ANTERIOR axillary line at the 4-5th intercostal space
- Place patient on nasal oxygen
- Antibiotics - Give one dose of intravenous cefazolin x 1 gram (Alternative: Clindamycin 600 IV)
- Pain control and sedation for patient
- Fentanyl, Morphine, Dilaudid, or Ketamine (in analgesic dosing)
- Consider procedural sedation with Ketamine
Tube InsertioN
The Procedure In Gif Format...
- Clean the insertion site with chlorhexidine or iodine.
- Create a sterile field by draping four sterile towels and a large sterile drape to frame the insertion site.
- Maintain sterile field throughout the procedure.
- Prepare the chest tube by cutting the external end to fit onto the atrium tubing and clamp it with Kellys.
- Anesthetize the skin and subcutaneous tissue. Too little anesthesia is the most common mistake.
- Start with the skin and subcutaneous tissue using lidocaine 1% with epinephrine.
- Advance the needle until it hits the rib inferior of the selected intercostal space and inject anesthetic over the periosteum. Then inject over the superior rib in a similar manner.
- While continuously aspirating, advance the needle over the inferior rib and into the pleural space (evidenced by return of air or blood). Withdraw the needle until the return of air ceases and inject onto the parietal pleura.
- Make a superficial skin incision, 1.5-2 cm in length, parallel to and overlying the rib inferior to the selected intercostal space.
- Create a subcutaneous track using Kelly clamps for blunt dissection.
- Keeping the Kellys in the closed position, advance over the inferior rib until the pleura is breached (confirm with “pop”/loss of resistance), then open the Kellys and withdraw them to create a tract.
- Insert one finger into the pleural space to confirm intrapleural location and rotate to identify lung and break up adhesions.
- Advance the chest tube into the pleural space using Kellys to guide it into appropriate position, anterior and superior for pneumothorax and posterior for hemothorax.
- Remove the Kellys and advance the chest tube to the appropriate depth.
- Confirm with chest radiograph before securing.
Securing the Tube
- Close half of incision with a single simple suture
- Place a second suture close to the thoracostomy tube
- Wrap remaining suture around tube to anchor and, leaving the ends long, tie down to the thoracostomy tube
- This tie will be cut upon removal of the tube and the long ends can be used to close skin after tube removal
- Occlusive dressing
- Cut a Y-cut into stack of 4x4 gauze ~2-3 layers thick
- Apply bacitracin/petroleum on one side of the gauze
- Place petroleum impregnated gauze around the thorocostomy tube with the petroleum against to the incision
- Apply 2-3, 4” by 8” tegaderm pieces over occlusive dressing to hold it in place
Full Videos of the Procedure

NEJM Tube Thoracostomy Video (Institutional Subscription Required)
Additional Options for Securing your Chest Tube
Dr. Omedary - Surgical Knot Tying:Drain Stitch. In this video I show you how to tie an easy drain stitch. Refer to my other videos for help with one and two-handed ties.
Emergency Trauma Management - How to Secure Your Intercostal Catheter/Chest Tube
Featured

Featured

References
- Kirsch, T. Tube Thoracostomy. Roberts and Hedges Clinical Procedures in Emergency Medicine. Ch. 10. 175-196.
- Gonzales RP and Holevar MR: Role of prophylactic antibiotics for tube Thoracostomy in chest trauma, Am Surg 1998, 64:617-620.




