Annals of B Pod: Phlegmasia Cerulea Dolens
/
Dr. Sobocinski takes us through a rare but interesting case of upper extremity swelling leading to limb ischemia caused by deep venous occlusion.
Read MoreDr. Sobocinski takes us through a rare but interesting case of upper extremity swelling leading to limb ischemia caused by deep venous occlusion.
Read MoreIn times of COVID, a Dimer of 3000 is nothing to look twice about, however there was an earlier (and future) time where the D Dimer is the hallmark of pulmonary embolism risk stratification. Dr. Comiskey breaks how how this once dichotomous tool has recent data to increase its specificity in elderly patients, pregnant patients and those with low pretest risk factors. Take a look, and when this whole pandemic is over your quiver will be fuller of Dimer tips.
Read MoreNot every swollen leg was made equal, nor should they all be treated the same. In the second installment of our case series, join us on the discussion of a rare vascular complication of the lower extremities.
Read MorePE is often a considered and easily risk-stratified diagnosis, however what about when you take away your definitive test of the CTPA? Dr. Ham examines the 60/60 sign and other ultrasonographic tests you can use to determine the acuity of right ventricular strain which is addition to the clinical and hemodynamic evaluation can help you triage additional strategies to traditional anticoagulation.
Read MoreIn this week's grand rounds, Dr. Stolz discussed all things DVT and the modified two-point compression study for lower extremity clots. In our recurring EM-neuro combined conference, Dr. Stettler discussed the recent DAWN trial results, and how to incorporate CT perfusion studies into our acute ischemic stroke decision trees. In our Quarterly Sim, we discussed the management of the crashing patient from a house fire, and practiced our escharotomy skills. In our mock oral boards, we went through cases on STEMI, carbon monoxide exposure and limb ischemia. Finally, Dr. Lane discussed the workup of acute diarrhea in the adult population, and Dr. Shah went through a particularly unique toxidrome presentation in his R4 Case Follow Up.
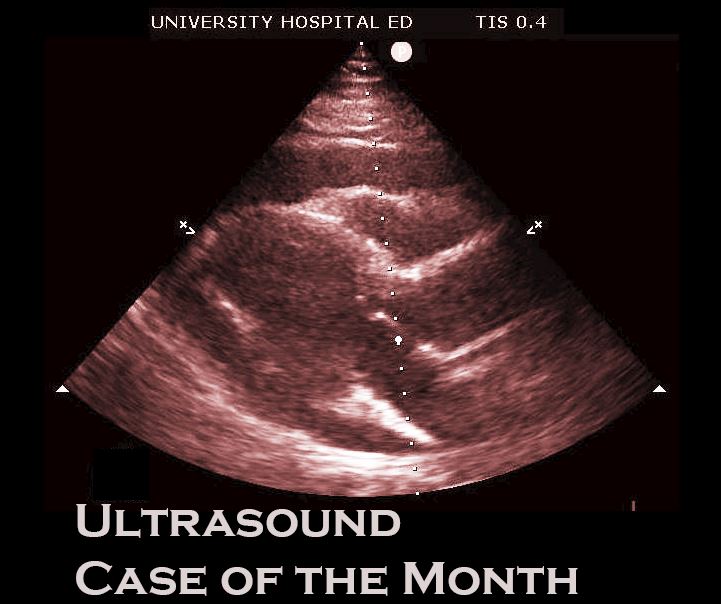
Read MoreIt's a frosty Easter morning and the ED is "q!&%t," all except for the 2 patient's turned over to you by the night ranger. You greet the first patient, a 75 yo M complaining of flank pain - probably a kidney stone you think to yourself as you walk in to the room. Walking into the room, you see the patient rolling around on the stretcher (as one would expect from those with a stone jammed in the UVJ), but something about his presentation strikes you as odd - a bit of diaphoresis, clammy pale skin. It could just be pain, but the specter of a ruptured abdominal aortic aneurysm still looms large in your differential diagnosis. You quickly exit the room, grab the ultrasound machine and head back in to take a look at his aorta...
Read MoreRemember that sometimes the thing a patient needs most is a specialist (i.e surgeon), especially trauma patients
SRU (pronounced "shrew") = Shock Resuscitation Unit
Training in, and managing, the SRU is one of the crown jewels of our residency. It is where the sickest of the sick patients are found in our ED. It is a crucible, a test of knowledge and strength, and a true manifestation of the tripartite mission of our department: Leadership, Excellence, and Opportunity.
Training in, and managing, the SRU is one of the crown jewels of our residency. It is where the sickest of the sick patients are found in our ED. It is a crucible, a test of knowledge and strength, and a true manifestation of the tripartite mission of our department: Leadership, Excellence, and Opportunity.