Grand Rounds Recap 9/30/2015
/
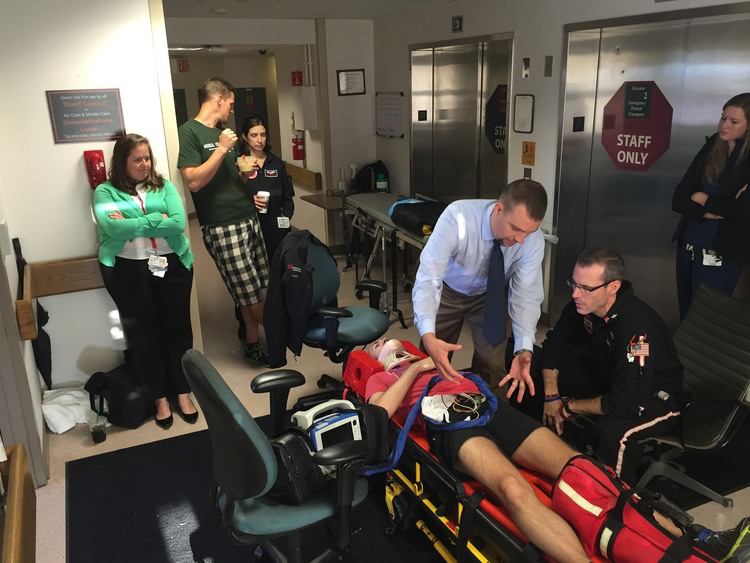
September Morbidity and Mortality Conference - Dr. Toth
Cases reviewed were from the month of August. We saw greater volume in 2015 than 2014 with longer ED hold times. We reviewed multiple cases including:
Acute Inflamatory Demyelinating Polyneuropathy
- Pain is a common presentation, and cranial nerve palsies are not infrequent, but they usually follow weakness and numbness of the extremeties.
- The diagnosis is in large part clinical, with progressive areflexia and sensory loss being the hallmarks. CSF studies showing albuminocytologic dissociation is confirmatory.